Background: Since the creation of Hospitalists in 1995, there has been much written about the importance of communication with primary care physicians (PCPs) as a routine staple of hospitalization. In practice, the inconsistent nature of hospitalist-PCP communication is well established. National surveys estimate the rates of communication to be between 20-40%. Amidst multiple barriers identified, not knowing whom to contact or how to contact is a persistent problem along with time and a perceived lack of benefit. The care of hospitalized patients on the wards at our 500-bed NYC Hospital is directed by the attending hospitalist, with either an advanced practice provider (APP) or a team of internal medicine residents. As recently as 5 years ago, some PCPs in the area were able to round on their ailing patients. With the transition to inpatient care being entirely supervised by hospitalists, many PCPs have reported a sense of frustration at the lack of a smooth transition from the hospital back to the office. Much of the frustration centers on medication errors.
Purpose: The goal of our project is to identify preferred modes of communication for the PCPs with the highest number of admissions to our service. The results will be used to improve existing Hospitalist- PCP communication practices at our institution.
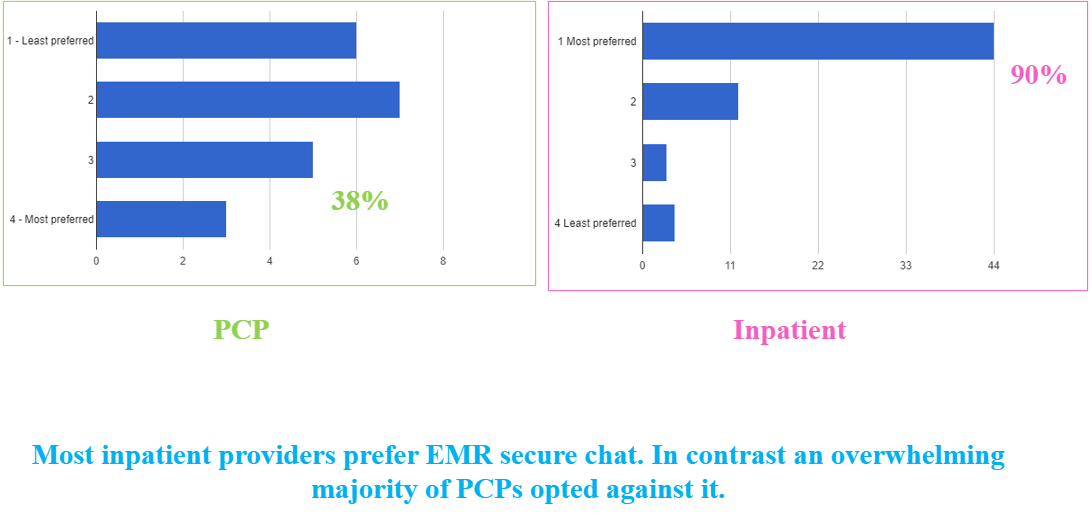
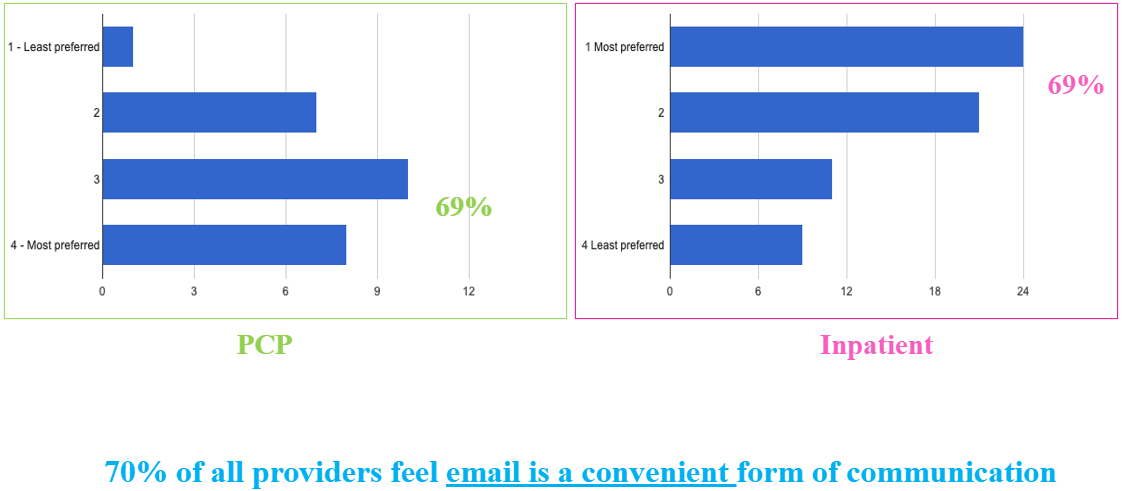
Description: We identified the top admitting PCPs by extracting data from the electronic medical record (EMR) for all hospital medicine admissions in 2019. Of the 12,458 admissions, 5854 did not have a PCP listed in the EMR, and 5813 were listed as “unspecified”. For the 791 patients with a listed PCP, those with the highest number of admissions and their partners in practice were included in our study. A questionnaire survey was sent to the ten highest admitting primary care practices, comprising a total of 57 PCPs in the community asking questions pertaining to preferred modes of communication. A mirroring survey was sent to inpatient providers including attending hospitalists, advanced practice providers, and internal medicine residents. Non-blinded questionnaire surveys utilizing a 4-point Likert scale of most preferred to least preferred methods were distributed via email. 32 of 57 PCPs (56%), 18 of 33 inpatient providers, including attending hospitalists and advanced practice providers (54%), and 48 of 143 internal medicine residents took the survey (33%). 66 % of PCPs and 50% of inpatient providers reported preference for EMR in-basket. An overwhelming 90% of inpatient provider’s listed secure chat as the preferred mode of communication as opposed to only 38% of PCPs. Nearly 70 % of all providers regarded email as a convenient form of communication. Both PCPs and inpatient providers agreed that office phone calls are an unfavorable form of communication. Finally, 30% of PCPs listed cell phone calls as their most preferred mode, but 63% of inpatient providers felt it was inconvenient.
Conclusions: We were able to identify differences in preferred modes of communication for PCPs, based on their practice type and access or the lack thereof to the EMR that is used in the hospital. EMR in-basket and email are the preferred modes of communication for all primary care practices within the same health care system. The PCPs who did not share the hospital EMR chose cell-phone or email as their preferred mode. Most of these comprise federally qualified health centers and solo practices. Unification of the EMR across varied medical practice settings would help improve PCP satisfaction during transitions of care.