Background: Misdiagnosis of catheter associated asymptomatic bacteriuria as CAUTI leads to inappropriate use of antibiotics and related consequences, including medication side effects, antibiotic resistance, C. difficile infection, and potential financial penalties to hospitals.
Purpose: To develop and implement an evidence-based pathway to improve evaluation of CAUTI in our academic health system.
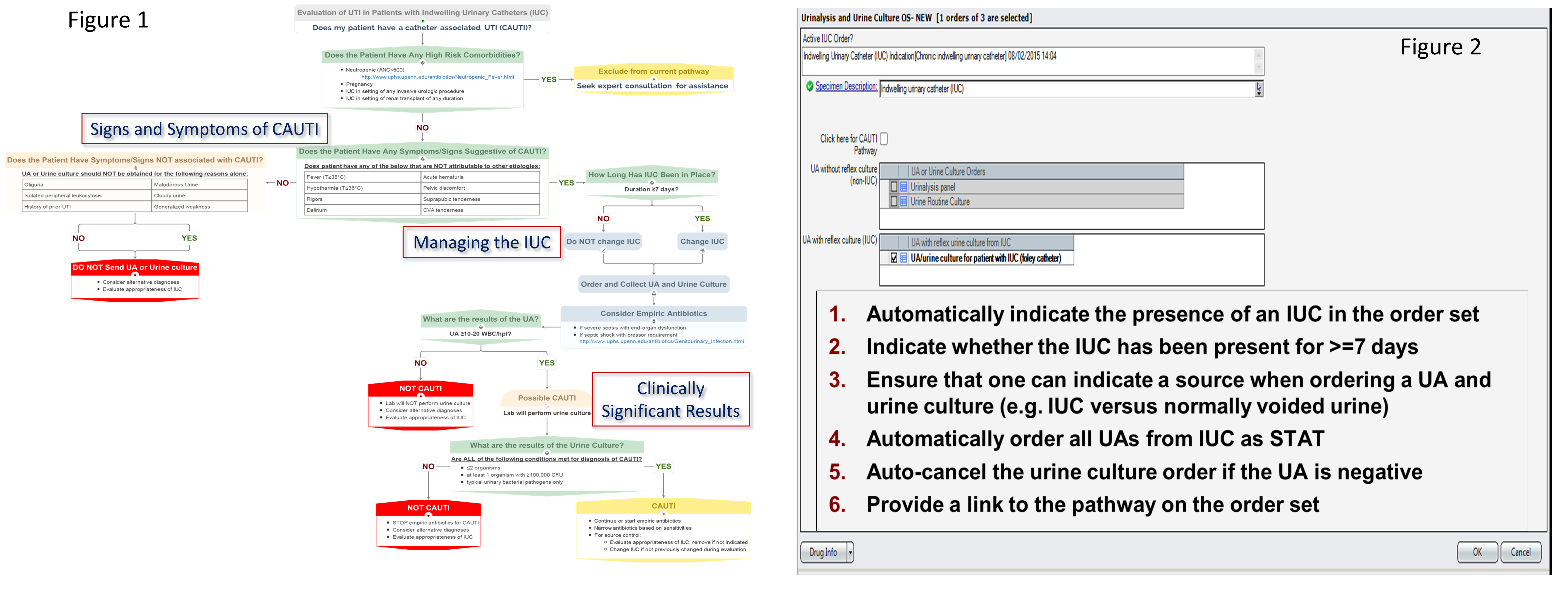
Description: Health system leadership identified the need to address the misdiagnosis of CAUTI at our institution. A multidisciplinary group of stakeholders including hospitalists, critical care, nursing, laboratory, infectious diseases, and informatics convened to develop an evidence-based pathway for the evaluation of CAUTI. Our hospital evidence-based practice center searched the literature to identify existing guidelines and pathways to inform the initial draft. The pathway was iteratively refined by the group until consensus was achieved (see Figure 1 for pathway details). Rapid systematic reviews were used to guide specific pathway decision nodes. Provider focus groups were assembled to understand providers’ knowledge and practices for the evaluation of CAUTI. They revealed knowledge gaps and variations in practice. A 13 item survey was also disseminated to assess baseline knowledge and practice patterns among housestaff, hospitalists, advanced practitioners (AP), and nurses in all critical care units in the month of October 2015. Response rates were approximately 50% for all respondent groups. The pathway was then implemented through a step-wise approach:
1) Education on the purpose and content of the pathway via standardized presentations by 2 housestaff champions at residency conferences for 5 programs, presentations by hospitalists at AP and nursing leadership grand rounds, and materials developed by 2 clinical nurse specialists for nursing education
2) Accessibility to pathway on an internal pathways website
3) Communication of the pathway using desktop screen savers and posters
4) Implementation of an order set in the electronic health record (see Figure 2 for order set features)
Conclusions: A CAUTI evaluation pathway was successfully developed and implemented using a multi-component intervention. Next steps are to evaluate pathway utilization rates by measuring website and order set use, pathway adoption by measuring impact on providers’ knowledge in a post-implementation survey, and changes in practice patterns by measuring ordered urinalyses, urine cultures, CAUTI rates, and antibiotic exposure in patients with indwelling urinary catheters (IUC).