Background: Prolonged hospitalizations for patients medically ready for discharge can increase healthcare costs, risk of complications, and strain on hospital capacity. Therefore, identifying and mitigating modifiable barriers to discharge that extend length of stay (LOS) is critical for improving quality of care.
Purpose: To address this challenge, the UNC Health Care Management Physician Advisor team initiated a project to gain a comprehensive understanding of discharge barriers contributing to prolonged length of stay (LOS). The objective was to develop and implement an electronic dashboard that identifies discharge barriers and factors prolonging LOS in currently hospitalized patients utilizing real-time electronic health record (EHR) data. The dashboard will provide a holistic view, enabling real-time monitoring, visualization, and quantification of factors and barriers for each hospitalized patient. Once modifiable discharge barriers are identified, targeted resource allocation and services can be implemented to effectively reduce LOS.
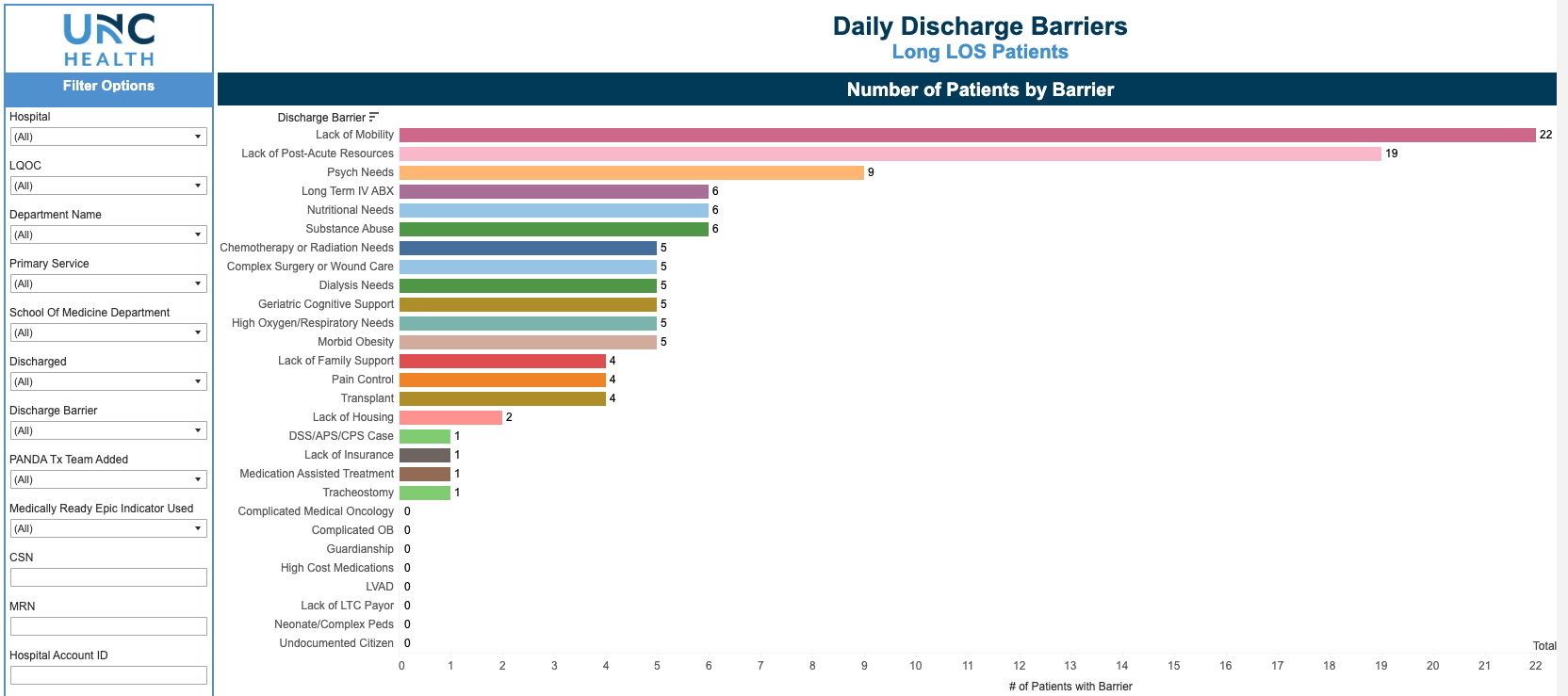
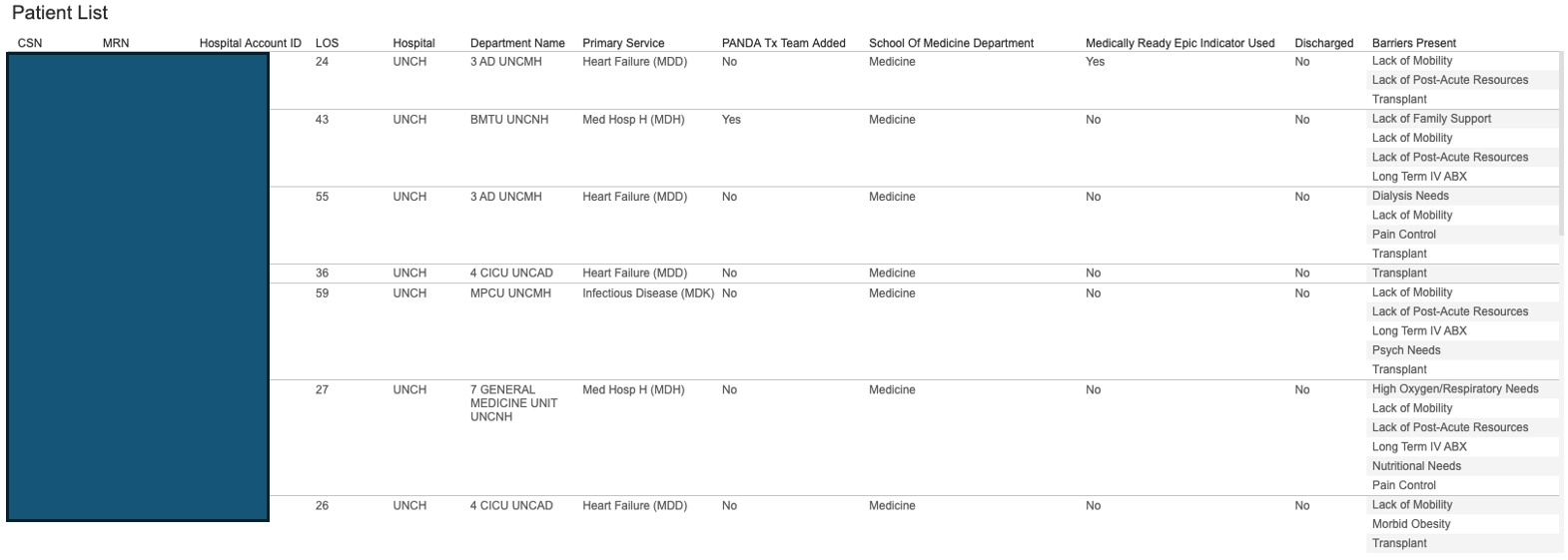
Description: Through manual chart review and expert consensus, 26 discharge barriers were defined and used to label a training and validation dataset. An analytical model was developed using structured and unstructured EHR data, and its outputs were visualized on a dashboard using Tableau. The training dataset included 1,239 long-stay hospitalizations. Common barriers associated with prolonged LOS included lack of mobility (56%), complex surgical wound care (45.7%), and nutritional needs (32.9%). Among patients deemed medically ready for discharge, lack of mobility (72.9%) and delays in post-acute resources (56.1%) were the most frequent barriers. The model demonstrated strong performance in detecting these factors, with an overall positive predictive value (PPV) of 0.70 and negative predictive value (NPV) of 0.99. Highest PPVs were observed for nutritional needs (0.92), complex wound care (0.86), and mobility deficits (0.82). Figure 1 shows a screenshot of the dashboard. Users can click on any barrier on the dashboard and get a real-time list of all hospitalized patients identified with the barrier (Figure 2).
Conclusions: The implementation of a real-time dashboard to track discharge barriers may provide an effective and scalable method to allocate and target resources to mitigate effects on LOS. Initial data from the dashboard resulted in allocation of 2 additional PT/OT resources in critical care settings at our hospital. Next phase of this project will focus on further testing of the model in different scenarios, adding in other services including pediatrics and psychiatry and possible integration of additional factors that impact LOS and discharge. We plan to operationalize the dashboard across our health system and evaluate its clinical implementation and impact on workflow and LOS reduction. Further refinement of our predictive model, including the integration of Natural Language Processing (NLP) algorithms, will enhance automated identification of prolonged LOS factors and discharge barriers from unstructured clinical notes. Additionally, continued collaboration with case management teams and health care leadership will be crucial in developing targeted interventions to address high-impact barriers, such as post-acute care access and functional mobility challenges.