
Background: Our health care system includes two academic medical centers (AMC) and community hospital locations. Occupancy at our AMC often exceeds 100%. Identifying patients while in the Emergency Department (ED) whose care needs can be safely and appropriately managed in a community hospital setting is a key priority. This approach helps preserved AMC capacity for patients requiring tertiary level resources, while improving access and care efficiency across the entire system. Previously efforts to identify and consent patients for transfer to a community hospital setting from an AMC ED location have achieved limited success.
Purpose: Our Hospital Medicine Unit (HMU) partnered with leadership from admitting, and ED administration leadership, to design a pilot program aimed at increasing transfers from AMC to community hospital setting by: improving the identification of patients eligible for community hospital level care, addressing potential barriers, increasing consent rates for patients eligible for transfer, and reducing the number of patients declined by the physician accepting transfers at the community hospital.
Description: The pilot was conducted for 4 weeks, Monday – Friday only. The pilot included key roles supported by both ED and hospitalist clinicians. An in person ED admin lead clinician role was scheduled from 7am to noon. This ED provider worked closely with ED colleagues to review medical boarders in the ED and help address any barriers to community hospital transfer. During peak admitting hours, 11am-11pm, a remote / virtual hospitalist shift reviewed all inpatient admission requests to Medicine or Cardiology services. Every admission was reviewed for eligibility to transfer to a community hospital setting, and when necessary the provider would conduct additional evaluation for any ambiguity or pending data. In addition, the hospitalist worked closely with consulting physicians to coordinate care across campuses, spoke directly with patients about their eligibility for care at the community hospital and helped communicate and coordinate with the receiving provider at the community hospital setting.Prior to the pilot, the average number of transfers to the community setting of 3.0 on weekdays and 2.9 on weekends, numbers which had remained stable for more than 3 years. During the pilot the average number of admissions on weekdays increased to 5.7, while on weekends (days not included in the pilot) the number remained unchanged at 3.1. Collaboration between the HMU, ED administration leadership, and Admitting led to a 36% increase in patient consents to community transfers and a 35% decrease in cancellations, with community hospital occupancy rising from 86% to 96%.
Conclusions: A collaborative model of ED and hospital medicine roles was successful at nearly doubling the number of AMC to community hospital transfers.
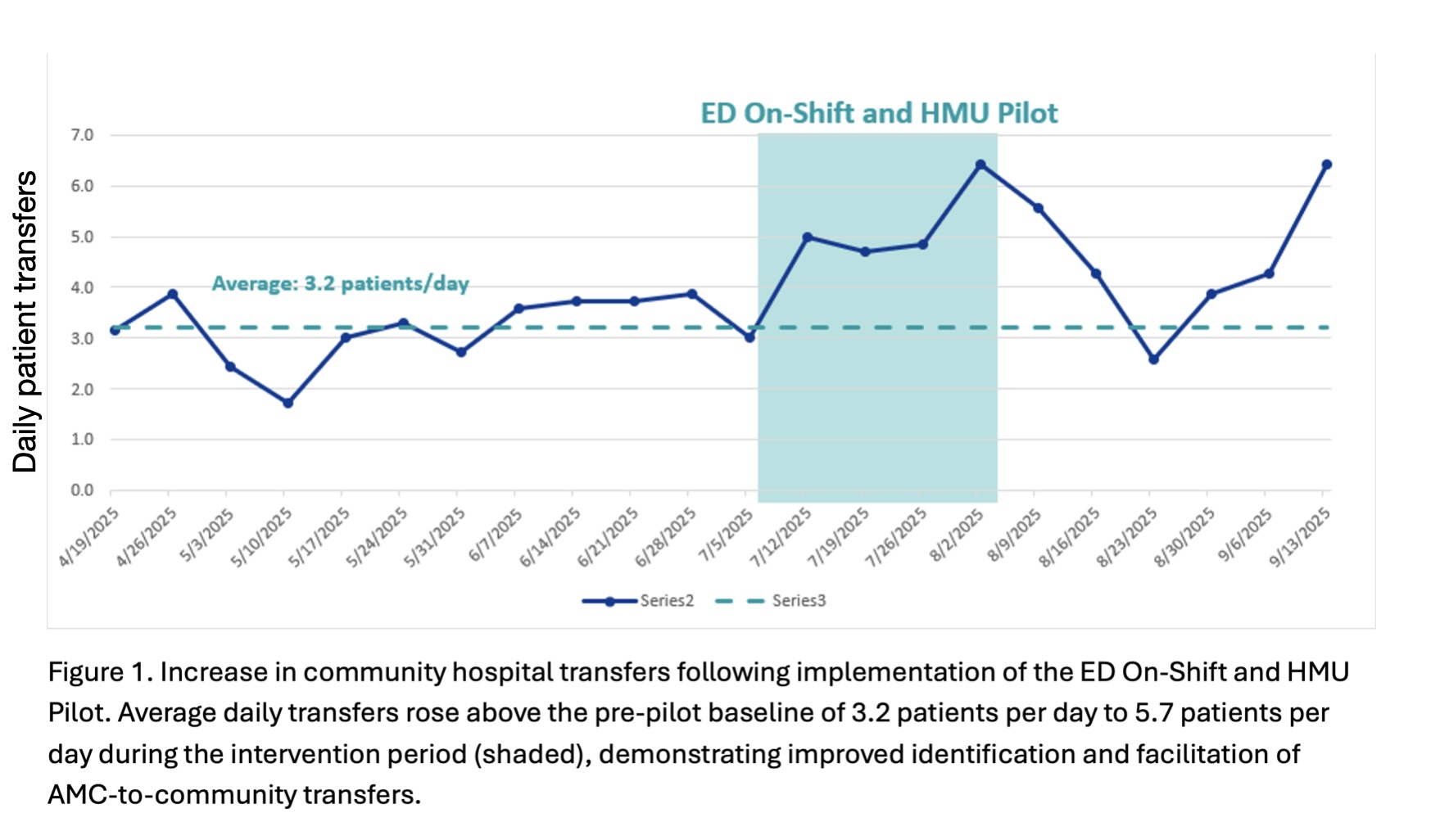
.jpg)