Case Presentation: A 21-month-old male with failure to thrive (FTT) presents to the ED with fever and poor oral intake. On exam, he was irritable but consolable, tachycardic with clear lung fields and no murmurs. CBC was within normal limits; electrolytes showed an anion gap metabolic acidosis attributed to dehydration. He was admitted to the pediatric inpatient unit for dehydration secondary to a viral illness and placed on IV fluids.
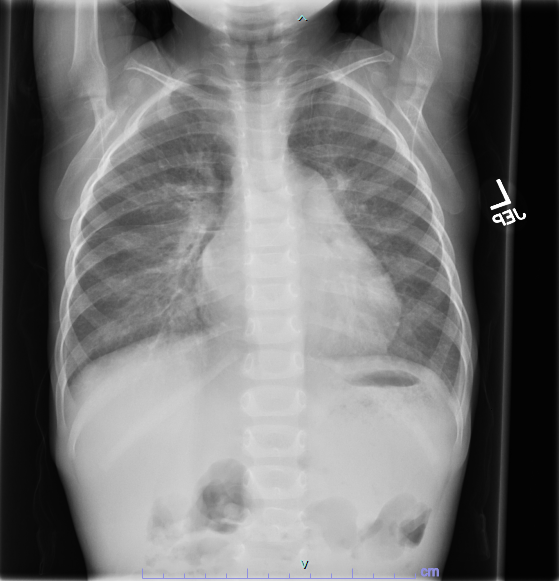
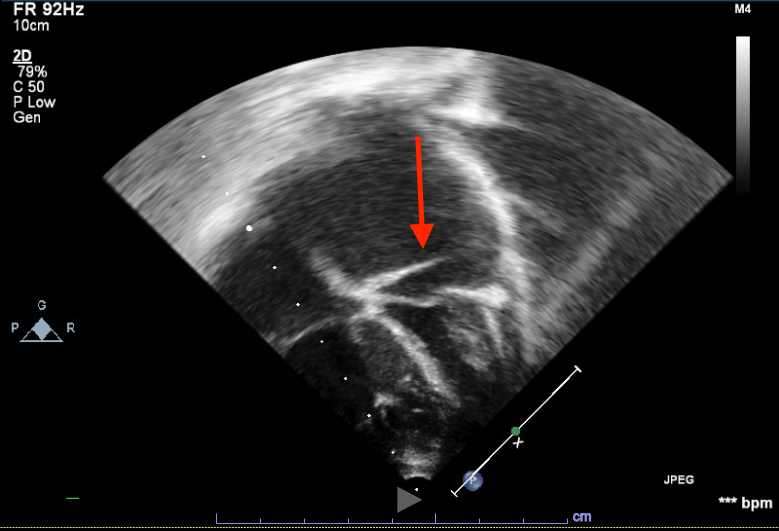
Due to FTT diagnosis, gastroenterology was consulted. Testing for food intolerances and malabsorptive processes was initiated which was unrevealing. He had 1.5kg weight gain over three days and developed facial edema, hepatomegaly and tachypnea, so IV fluids were discontinued. Chest x-ray showed pulmonary venous congestion, ECG revealed possible left atrial enlargement, and BNP was elevated at 2,286 pg/mL. Echocardiogram revealed cor triatriatum sinistrum. Pediatric cardiology was consulted, and the patient was diuresed with furosemide. After reaching euvolemia, he was discharged home and followed closely. He underwent surgical resection of left atrial membrane. Post-operative course was uncomplicated and FTT resolved.
Discussion: Cor triatriatum sinistrum (CTS) is a rare heart defect, and may be associated with other cardiac defects. Embryologically, CTS is attributed to failure of the common pulmonary vein being incorporated into the left atrium. This results in functional division of the atrium into two chambers by a thin fibromuscular membrane which causes a variable, and sometimes progressive, obstruction of flow in the left atrium.
CTS may present at nearly any age, with cases of more severe obstruction presenting during infancy. Typical presenting symptoms include activity intolerance, cyanosis, respiratory distress, murmur, and cardiogenic shock. In this case the pulmonary venous congestion resulted in symptoms of tachypnea and FTT more commonly seen with pulmonary over circulation in left to right shunts such as ventricular septal defects. Diagnosis may be made with transthoracic echocardiography.
Treatment of CTS is surgical resection with excellent outcomes, particularly if identified early and without associated cardiac defects.
Conclusions: Cor triatriatum is a rare congenital heart defect that typically presents with cyanosis, activity intolerance or respiratory distress, but may present with FTT. Although less typical for presentation, it is important to consider cardiac etiologies in the differential diagnosis of FTT, particularly in patients with evidence of pulmonary venous congestion even in the absence of murmur.