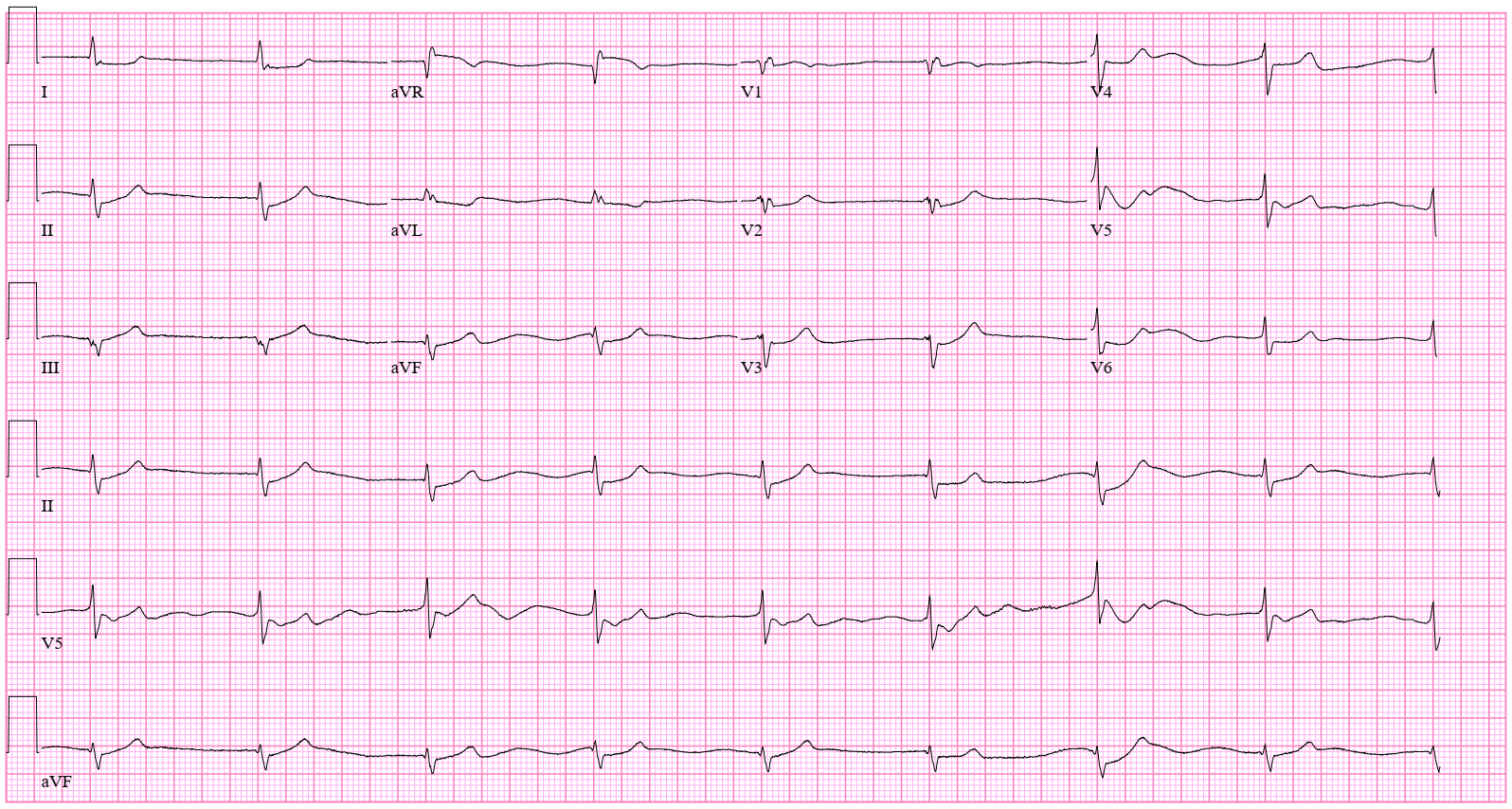
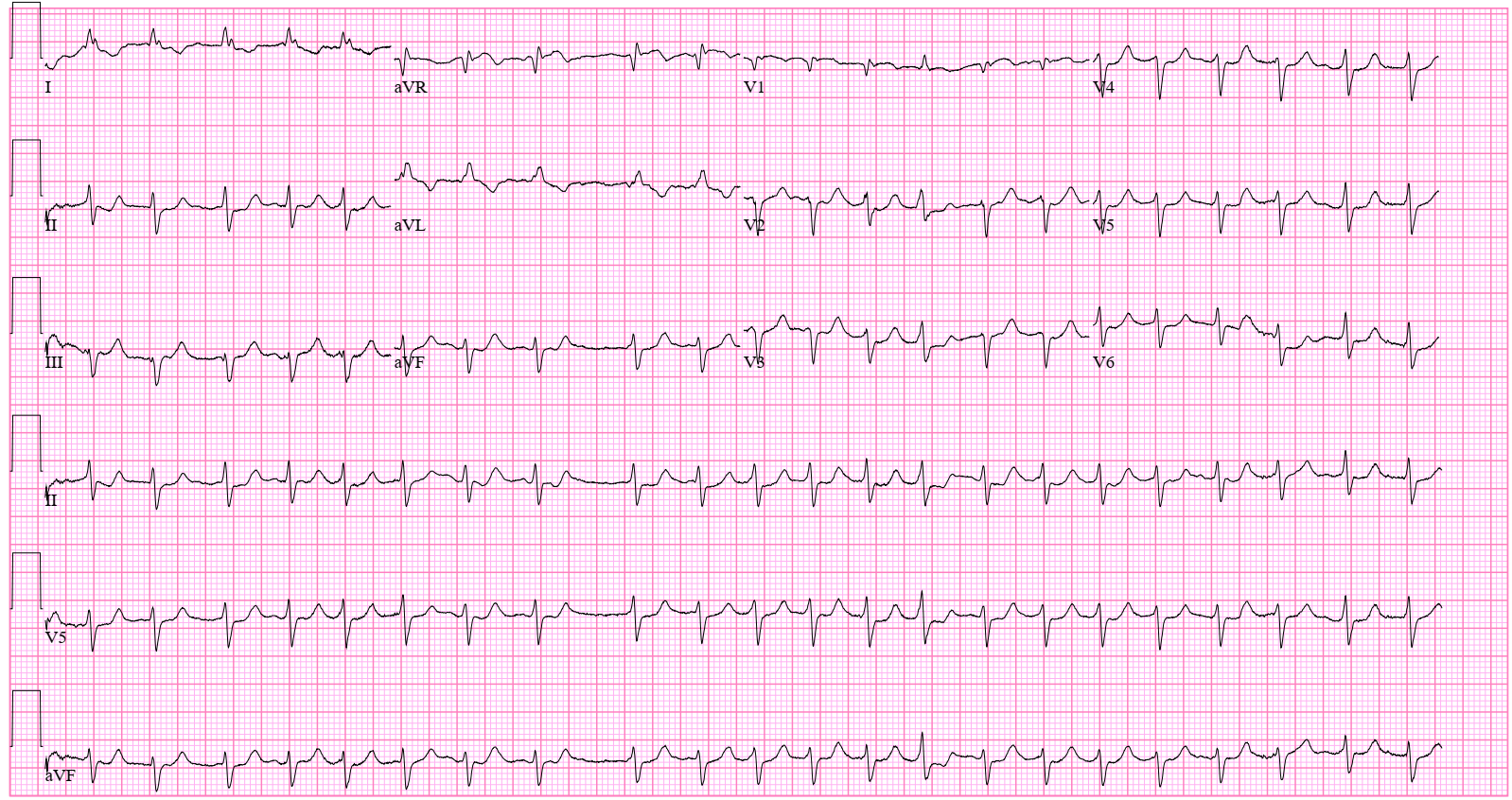
Case Presentation: 56-year-old Caucasian male with history of atrial flutter/fibrillation, heart failure with preserved ejection fraction, coronary artery disease status post coronary artery bypass graft surgery, mechanical aortic valve replacement presented to the emergency department with progressive generalized weakness, fatigue and shortness of breath for 5 days. He was on metoprolol and verapamil for rate control of atrial flutter/fibrillation. However, due to his borderline normal pressure and inadequate rate control, he was started on digoxin two months ago. On admission, patient was noted to be hypotensive and bradycardic (blood pressure 87/54 mm Hg, heart rate 50 beats/min). Initial labs remarkable for elevated creatinine of 4.86 mg/dL (baseline creatinine-0.6 mg/dL) consistent with acute kidney injury. He had normal serum potassium and magnesium levels. Troponin was negative. Electrocardiogram (ECG) showed new junctional rhythm with depressed and concave ST segment typical of “digoxin effect”. Transthoracic echocardiogram showed normal ejection fraction, without any wall motion abnormalities. Serum digoxin level was obtained and found to be normal at 1.0 ng/mL. He received fluid boluses and was started on intravenous norepinephrine infusion. However, he remained bradycardic with heart rate at 50 beats/min. Digoxin toxicity was suspected due to persistent bradycardia and ECG abnormalities. Patient was administered antidotal therapy with DigiFab. Few hours after administration of DigiFab, his heart rate improved and he was in atrial fibrillation with rapid ventricular response requiring amiodarone infusion. He was later discharged on amiodarone and metoprolol.
Discussion: Digoxin toxicity can occur with precipitating factors such as renal dysfunction, hypokalemia, hypomagnesemia or drug interactions (especially non dihydropyridine CCBs). Clinical features of digoxin toxicity commonly include neurologic manifestations such as lethargy, fatigue, confusion, visual disturbances and gastrointestinal symptoms such as nausea, vomiting, diarrhea and abdominal pain. Almost any arrhythmia can occur with digoxin toxicity and premature ventricular contractions are the most common. Others include bradycardia, atrial tachyarrhythmias with AV block, junctional rhythms, ventricular tachycardia, and ventricular fibrillation. Our patient has digoxin toxicity, despite normal digoxin levels, which likely happened in the setting of his renal dysfunction and verapamil use.
Conclusions: Serum digoxin concentration may not necessarily correlate with toxicity. This case emphasizes that digoxin toxicity can occur in patients with normal digoxin and potassium levels and the diagnosis of digoxin toxicity should be based upon clinical and electrocardiographic manifestations, not serum digoxin level.