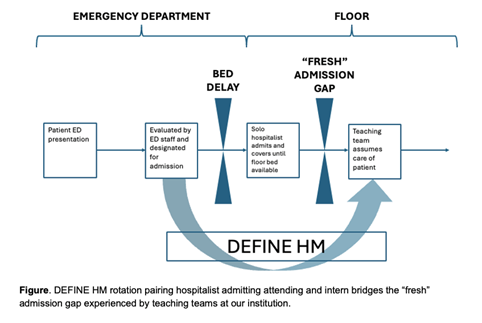
Background: Access to “fresh” admissions, in which an admitting team is the first to evaluate a new patient apart from emergency department (ED) staff, is critical to the experience and skill development of medical trainees, particularly interns. Fewer fresh admissions were assigned to teaching teams at Yale New Haven Hospital between 2019-2021 due to system-level factors, high ED census, high inpatient medicine census, and complex discharge barriers. Decreased throughput resulted in patients waiting long periods in the ED, and a de-localized hospitalist admitting team was successfully employed to initiate care for ED boarding patients. Teaching teams frequently inherited the care of these already-admitted patients once assigned a bed outside of the ED, thus opportunities to admit fresh admissions were limited.
Purpose: Our purpose was to bridge the gap between medical trainees and the need for fresh ED admissions, with the goal of increasing exposure to patients with undifferentiated diagnoses in a 1:1 attending-to-intern learning environment. Prior studies demonstrate increased resident satisfaction regarding hospitalist-led inpatient teams with benefits including increased learner autonomy, increased awareness of cost-effectiveness, quality measures, and confidence/preparedness for future rotations and career goals. This innovative rotation, predicated on direct observation and real-time coaching, leverages these advantages while providing learners with the opportunity to focus on the initial diagnostic approach to common medical presentations.
Description: We designed and implemented a novel 2-week inpatient rotation at Yale New Haven Hospital called Direct in ED Care for Interns Experience in Hospital Medicine (DEFINE HM). This is a two-physician teaching admitting team composed of an attending hospitalist and intern tasked to admit new patients directly from the ED. The learning dyad has no other cross-coverage clinical responsibilities and focuses on important clinical skills such as triage, rapid intervention, and the initial diagnostic evaluation. This structure allows for real-time observation, feedback, and coaching. The dedicated focus on the admission process of care also allows for essential systems-based learning skills such as detailed admission medication reconciliation and the use of electronic medical record (EMR)-integrated clinical pathways. The rotation curriculum is primarily case based and can be tailored to observed learner needs. We also include built-in content on patient safety and a structured, protected time for supervised procedures.
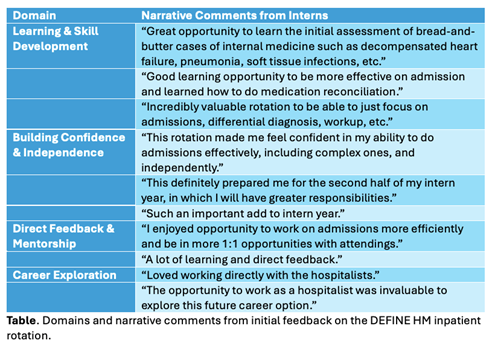
Conclusions: This rotation has proved successful as a highly valued rotation. Summative feedback to date has been overwhelmingly positive, receiving praise as a novel, sustainable means for incorporating junior learners into direct care models. Themes identified in narrative comments from interns include learning and skill development, building confidence and independent, direct feedback and mentorship, and career exploration. The DEFINE HM clinical experience creates a unique opportunity for learners in an immersive environment, free from floor-based responsibilities and interruptions. Given national boarding crises in EDs, other programs may benefit from creating dedicated admitting rotations for learners. While our structure is unique given the pre-existing dedicated admitting attendings protected from other clinical responsibilities, this structure can be adapted to a range of local staffing models.