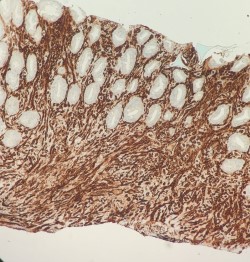
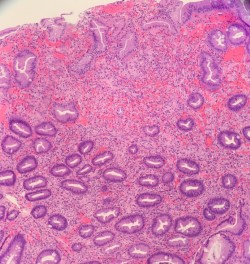
Case Presentation: The patient is a 54 year old man with PMH of HIV (non adherent to medications) who presented with worsening cough, was hemodynamically unstable, and did not respond to fluid resuscitation initially. Hemoglobin was found to be 6, platelets 29. He was transfused 2 units of pRBC and 1 unit of platelets, Hb responded appropriately. Sepsis was thought secondary to PNA or other to be identified infection. His acute anemia was concerning for GIB, he had multiple bloody bowel movements. Labs were remarkable for a CD4 count of 13, with a HIV RNA viral load of 3.78 million, as well as profound pancytopenia. HAART was started. There was concern for AIDS defining illness as etiology of patient’s presentation, given his lab work up. CT head was negative for acute brain pathology. Flow cytometry study was inconclusive and pathology was consistent with changes related to viral infection rather than neoplastic process. CMV was negative. Brochoscopy confirmed HHV-8 present. Sigmoidoscopy showed a fungating mass suspicious for Kaposi Sarcoma, biopsy was confirmed via pathology. Over the hospital course, Hb ranged from 6-9, platelets from 22-64. Overall the patient required 7 units of pRBCs and 23 units of platelets, and was given 3 units FFP. Final diagnosis was disseminated Kaposi Sarcoma confirmed by biopsy as above mentioned (colon, lung). After the patient was stabilized, transfer was arranged to NIH Cancer Center in Bethesda specialized in the treatment of Kaposi’s Sarcoma.
Discussion: Disseminated Kaposi’s sarcoma (KS) has become relatively rare in the U.S. since the advent of HAART with about 6 cases per million per year. Of those, approximately 1 or 2 will have visceral manifestations/dissemination of disease. The most common visceral spread is to the gastrointestinal tract and lungs, their mucosal lining a hub for HHV-8, the viral culprit linked to KS. In addition to beginning HAART if not already in place, treatment for disseminated disease is chemotherapy, with paclitaxel or a liposomal anthracycline. Management was challenging, the patient requiring multiple blood product transfusions, diagnostic and therapeutic procedures while relatively unstable, and careful attention to balancing his poor immune function with the needed drug treatments.
Conclusions: In the 1980s, homosexual men with AIDS were by far the largest group of those with Kaposi’s sarcoma to be afflicted with the most aggressive and fatal forms of the disease, which was to become one of the AIDS defining illnesses. The 1990s brought with it the discovery of the link between Kaposi’s sarcoma and HHV-8- the great majority of KS lesions (>95%) have evidence of HHV-8 infection, cementing that it is key in the pathology of KS. It was also in the 1990s that HAART became available, and would finally make a large impact on the prevalence of AIDS defining illnesses over the years. Yearly KS cases have now been essentially reduced by 87% from their highest point in the nineties. Of course, the immune deficiency that HIV/AIDS brings with it plays a leading role in acquisition of KS disease, it follows that better control of the disease with modern drugs has been the primary factor in reducing reported cases. Hospitalists encounter cases of disseminated Kaposi’s sarcoma infrequently but given the severity of the disease, it remains imperative to be aware of AIDS defining illnesses and their management. Our patient provides a window into the process of diagnosing, treating, and managing this devastating disease that has now become exceedingly rare in the United States.