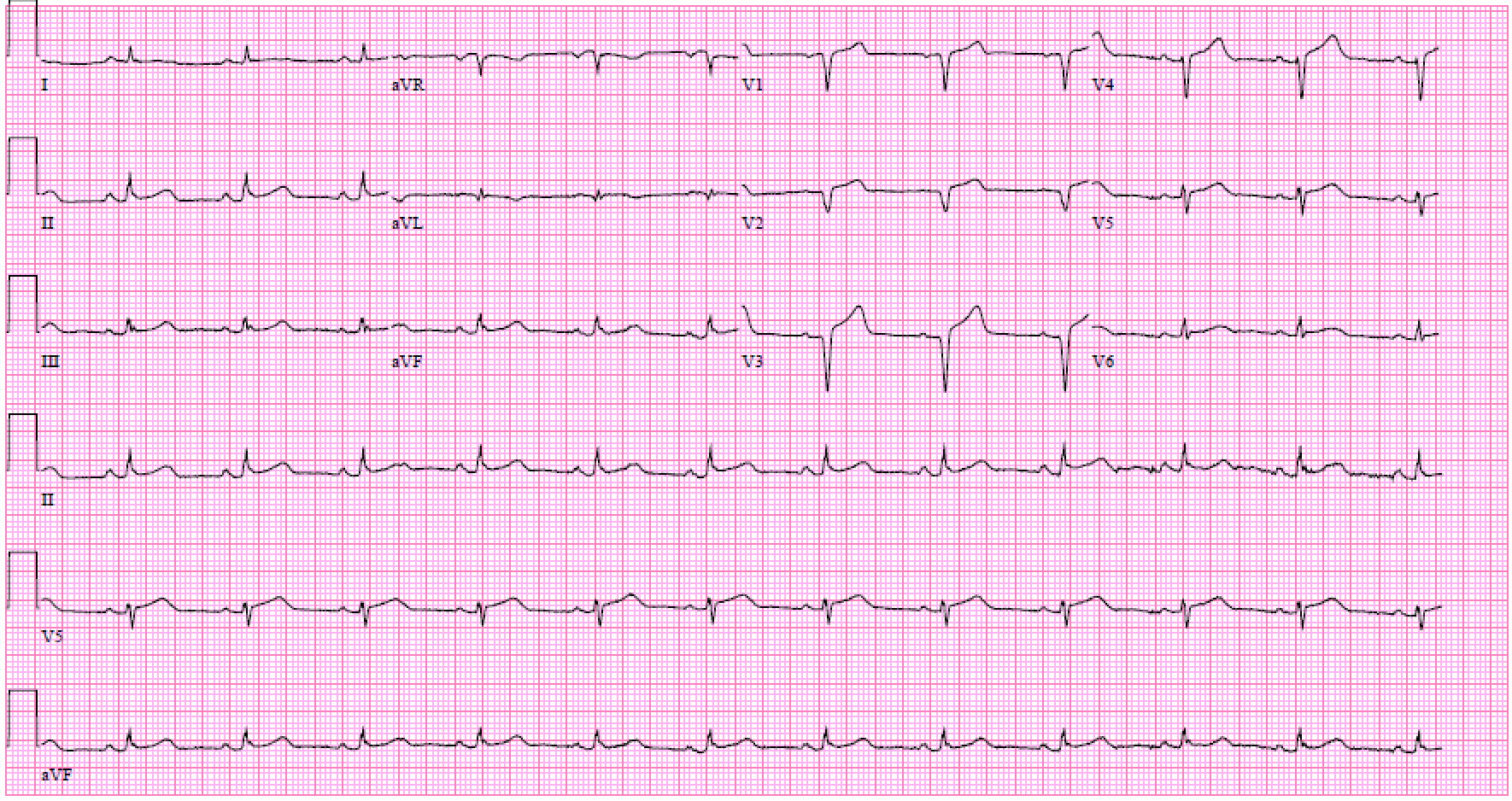
Case Presentation: A 67 year old male with a past medical history of recurrent pericarditis, hypertension, psoriatic arthritis, and gout presented with diffuse chest pain. Patient stated that the pain was substernal, 10/10, sharp in nature, and non-radiating. Pain was aggravated by exertion and alleviated with rest, nitroglycerin and morphine. Pain was associated with shortness of breath, nausea, and diaphoresis. Patient notes that he has had 7 episodes of pericarditis in the past, and the pain/pressure was similar nature to those episodes. Patient reported having a cardiac catheterization 1-year prior that showed a 40% LAD occlusion. On arrival, EKG was done which showed diffuse ST segment elevations. Initial troponin was 0.7. Patient was initially diagnosed with pericarditis and started on colchicine and prednisone, with the thought that it was autoimmune in nature. Troponin subsequently trended up to 8.58, which was interpreted as possible conversion to myocarditis. Troponin persistently increased to 37.1. Echo was obtained which showed, a nondilated left ventricle with an akinetic entire apex, mid anteroseptal and mid inferoseptum and mildly decreased systolic function. The estimated left ventricular ejection fraction was 40%. Wall motion abnormalities were consistent with either infarction in the LAD distribution or takotsubo cardiomyopathy. Patient was taken for cardiac catheterization. Patient was found to have 100% occlusion of the LAD mid segment and two drug-eluting stents were administered. It was noted that this patient had wraparound LAD anatomy. The diffuse ST elevations seen on EKG were thought to be secondary to wraparound LAD.
Discussion: Pericarditis is a condition defined by inflammation of the pericardial sac. Certain coronary artery anatomical variations can present a challenging diagnostic consideration of ST elevation myocardial infarction with diffuse ST elevations on EKG mimicking pericarditis.
Conclusions: In the “Usefulness of the Left Anterior Descending Artery Wrapping Around the Left Ventricular Apex to Predict Adverse Clinical Outcomes in Patients With Anterior Wall ST-Segment Elevation Myocardial Infarction”, an INFUSE-AMI Substudy the “Wraparound LAD” was defined as an LAD reaching the apex and supplying the apical inferior aspect of the heart. Among the total 338 patients in this study, 258 (76.3%) had wraparound LADs. With this significant number of potential patients presenting with wraparound LAD anatomy this case illustrates a critical consideration in the diagnosis and management of patient with presumed diagnosis of pericarditis or myocarditis in which ST segment elevations are seen diffusely on EKG. Trending troponin, serial EKGs and an early echocardiogram are of paramount importance in order to not miss an underlying STEMI with wrap around LAD distribution.