Background: Initial management of acute upper gastrointestinal bleeding (UGIB) aims towards aggressive fluid resuscitation to maintain hemodynamic stability. Existing evidence regarding benefit of early endoscopy is unclear with some studies suggesting mortality benefits and some suggesting otherwise. The purpose of this study is to evaluate if there is any mortality benefit of doing early endoscopy within 24 hours of presentation.
Methods: From July 2013 to July 2016, 179 patients admitted with a diagnosis of non-variceal UGIB were retrospectively reviewed. Clinical variables including 30-day mortality were then compared between the patients who had endoscopy within 24 hours with those who had endoscopy after greater than 24 hours.
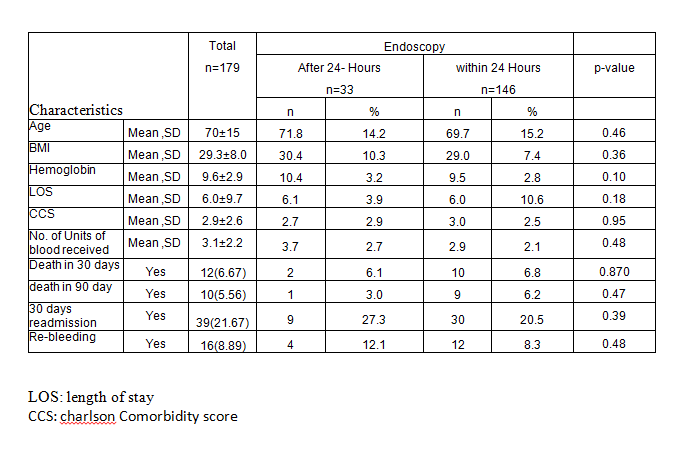
Results: Out of 179 patients admitted for non-variceal UGIB, 146 underwent endoscopy within 24 hours and 33 underwent it after 24 hours of presentation. The overall mortality associated with UGIB was 6.6% (12/179). There was no statistically significant difference found in 30-day mortality among the two groups (6.8% within 24 hours vs 6.1% after 24 hours). There was also no difference in 30-day readmission (20.5% within 24 hours and 27.3% after 24 hours) and rates of rebleeding among the two groups (8.3% within 24 hours vs 12.1% after 24 hours). The length of stay was also similar in both groups (6 days vs 6.1 days).
Conclusions: This study did not find any advantage of early endoscopy within 24 hours on length of stay, rate of complications and 30-day mortality. As hemostasis is achieved in almost 90% of patients with supportive management without any endoscopic intervention, focus should be made on aggressive fluid resuscitation as it has a clear mortality benefit.