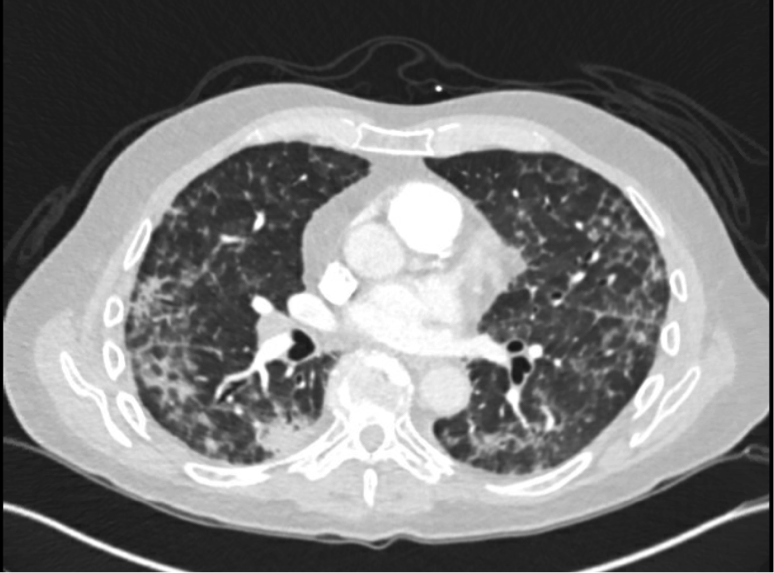
Case Presentation: A 68-year-old male with a medical history of gastrointestinal stromal tumor (GIST) on Imatinib and paroxysmal atrial fibrillation on Apixaban presented with a 4-week history of progressive dyspnea. He had outpatient evaluation for these symptoms previously at which time COVID-19 testing was negative and chest radiography findings were consistent with pneumonia. He was started on Doxycycline for anti-microbial coverage. In the interim, anti-microbial coverage was broadened to Amoxicillin-Clavulanate and a second testing for COVID-19 was negative. At a subsequent visit, he was hemodynamically stable, but hypoxic and requiring 3L of supplemental oxygen via nasal cannula requiring admission. On examination, his breathing was labored, tachypneic and appreciable for scattered rhales throughout bilateral lung fields. A computed topography angiography (CTA) of the chest revealed diffuse bilateral ground glass, nodular alveolar and reticular opacities with areas of subpleural sparing with no evidence of pulmonary embolism. He was empirically started on Vancomycin and Piperacillin/Tazobactam for hospital acquired pneumonia (HAP) coverage. Initial laboratory evaluation including a complete blood count, BNP, procalcitonin, HIV, streptococcus pneumoniae and legionella urine antigen testing were unremarkable. Echocardiogram revealed a normal systolic function with no other abnormalities. A bronchoscopy with bronchoalveolar lavage (BAL) found no bacterial, fungal or acid-fast organisms on culture and viral studies were negative. Antimicrobial therapy was discontinued, and the patient was started on IV Solumedrol for Imatinib-induced pneumonitis. He had clinical improvement and was discharged home on a steroid taper.
Discussion: Gastrointestinal stromal tumors (GIST) comprise the most common mesenchymal malignancies of the gastrointestinal tract and likely originate from the interstitial cells of cajal. Approximately 80% of GIST’s have deregulation of C-KIT leading to over-expression and gain of function mutations. Diagnosis is confirmed by immunohistochemical analysis of KIT+, CD34+ and DOG1+. Imatinib mesylate is a tyrosine kinase inhibitor that specifically targets C-KIT and halts tumor proliferation. It is now preferred for locally advanced disease, metastatic disease, and neoadjuvant therapy in the treatment of GIST. Most common adverse effects include nausea, vomiting, diarrhea, myalgia, skin rash and edema whereas pneumonitis or pulmonary fibrosis are exceedingly rare. The exact pathogenesis is unclear, but may be an immune complex-mediated reaction progressing from acute alveolitis to pneumosclerosis. Imatinib-induced pneumonitis develops 10 to 282 days following initiation, with a median time of 49 days and a dose range of 200-600mg daily. Treatment involves discontinuation of Imatinib followed by corticosteroid therapy.
Conclusions: Drug-induced pneumonitis is a rare adverse effect with Imatinib therapy. Diagnosis can be delayed and challenging given the presence of non-specific symptoms including cough, dyspnea or malaise with chest imaging showing interstitial pulmonary infiltrates. Prompt evaluation and identification is imperative with the initiation of corticosteroid therapy to circumvent progression of lung disease. This case reinforces the importance of hospitalists considering medication-induced causes in their differential diagnosis.