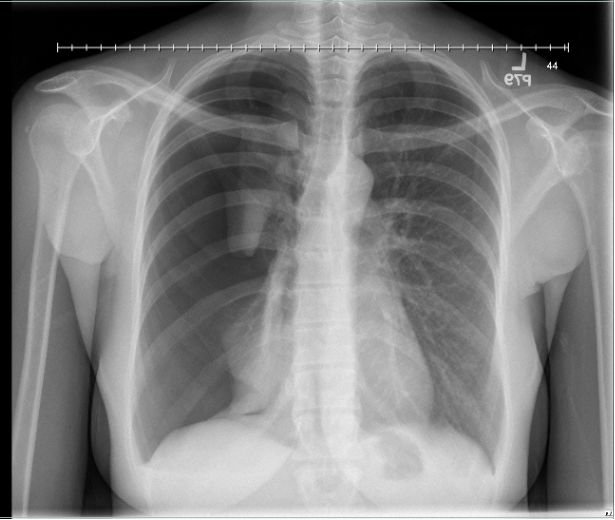
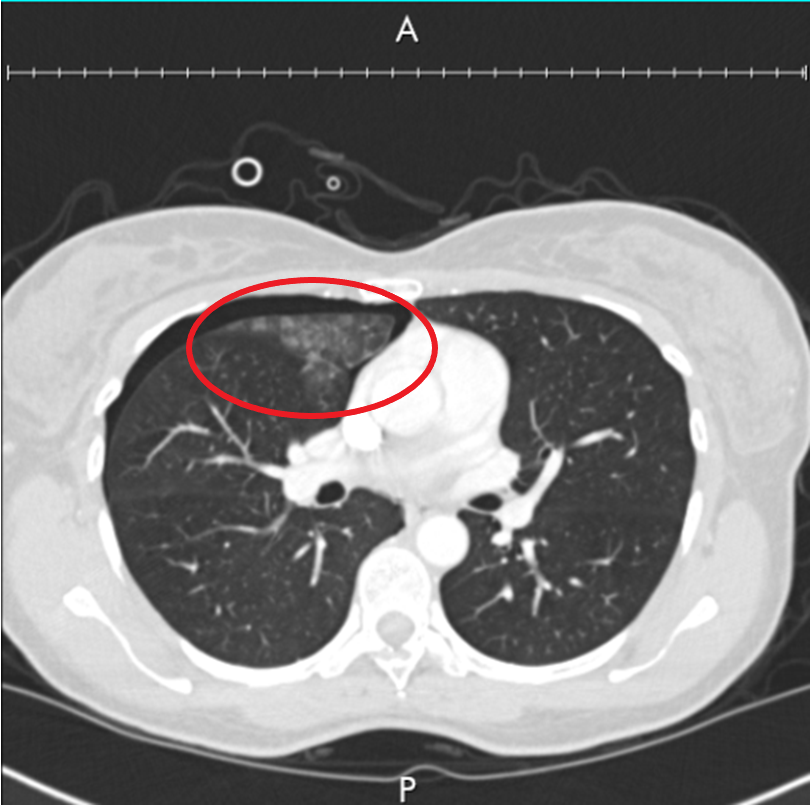
Case Presentation: A 38-year-old female presented to the emergency department with sudden-onset sharp right-sided chest pain and shortness of breath, associated with exertion at work. Notable medical history included recurrent episodes of brief dyspnea starting one day before her menstrual period and subsiding 1-2 days later. At the time of admission, the patient was on the second day of her menstrual cycle. The patient reportedly had a history of recurrent chest pain and dyspnea associated with menses and a remote history of pneumothorax while on oral contraceptives. She denied any other medical history, including known pulmonary disease. She denied tobacco abuse but did endorse secondhand smoke exposure. Relevant family history included a father with lung cancer associated with tobacco use. Initial chest X-ray (Image 1) on admission revealed a right-sided pneumothorax with complete collapse of upper and lower right lobes. A chest tube was subsequently placed in the right pleural space for management. CT scan of the chest (Image 2) revealed ground-glass opacities concerning for parenchymal hemorrhage on the anterior aspect of the right upper lobe of the lung. Catamenial pneumothorax was suspected due to her history of chest pain and dyspnea associated with menses. Although her pneumothorax resolved with the chest tube, video-assisted thoracoscopic pleurodesis was performed for definitive management. The procedure revealed small diaphragmatic fenestrations, which were resected. She was also found to have dark purple marks on the right lung’s lower lobe, concerning for endometrial tissue. The patient was safely discharged two days post-operatively.
Discussion: Catamenial pneumothorax is a rare disease in women in which recurrent spontaneous pneumothoraces occur in association with the menstrual cycle [1]. Recognition and treatment of catamenial pneumothorax in the inpatient setting can be challenging, given the varying symptoms and presentations of pneumothorax. Our patient’s history of recurrent dyspnea associated with menses and previously diagnosed pneumothorax were the initial tip-off for her catamenial pneumothorax diagnosis. Initial imaging followed by Video-Assisted Thorascopy was proven useful in further supporting this diagnosis.
Conclusions: There are multiple theories on the exact pathogenesis of catamenial pneumothorax, but there is no universally agreed-upon mechanism. Diagnosis is generally clinical and can be made if pneumothorax is found 72 hours before or after the start of menstruation with confirmation through a combination of clinical history, imaging, and direct visualization modalities such as video-assisted thoracoscopy [2,3]. From the management of this patient, if a premenopausal patient presents with cyclical symptoms of pneumothorax associated with menses, catamenial pneumothorax should be on the differential.