Background: The use of opioids postoperatively is becoming common practice to achieve pain relief. The goal of the perioperative period is to relieve suffering, achieve early mobilization after surgery, and reduce length of stay (LOS). Often opioids, are prescribed without trying alternative methods for pain relief. There is a growing concern for overuse of opioids in the United States and worldwide due to the misuse and overprescribing. Ineffective pain management is associated with increased complications and a longer LOS. The optimal strategy for perioperative pain control consists of multimodal therapy to reduce opioids. Postoperative pain is often managed with opioids. This can be associated with respiratory depression, excessive sedation, and severe constipation (ileus or obstruction) that may delay hospital discharge. The administration of intravenous (IV) acetaminophen (Ofirmev) may balance the control of postoperative pain while reducing opioid consumption and LOS. Guidelines for management of acute pain include round the clock non-opioids in addition to opioids. The available IV preparation is significantly more expensive than the oral acetaminophen. Currently, Ofirmev is approximately thirty-five dollars per dose.
The purpose of this investigation was to determine whether Ofirmev can reduce the opioid requirement and LOS in post-surgical patients to offset the additional cost of IV acetaminophen. The secondary purpose will investigate if Ofirmev plus concomitant non-opioid medications have synergistic effects compared to Ofirmev alone.
Methods: A retrospective case control chart review performed on surgical patients who received at least two (2) doses of Ofirmev (1 gram every 6 hours) between April 2013 and April 2017 compared with surgical patients (control group) who did not receive Ofirmev for postoperative pain between March 2009 to March 2013 (before Ofirmev was added to formulary). Demographic information, co-morbidities, surgical history, allergies, and type of procedure, details on medications administers, and LOS collected.
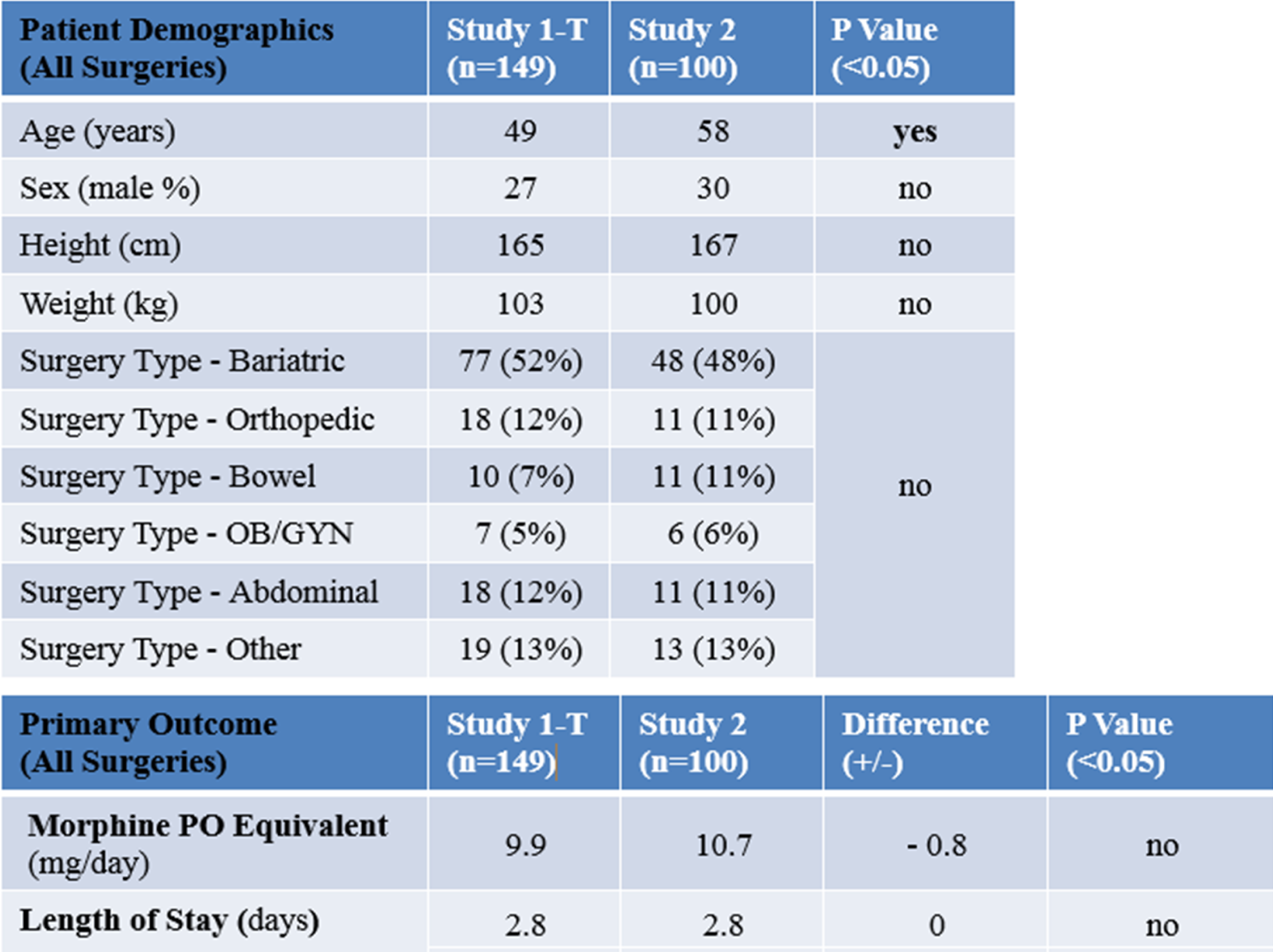
Results: There were two study groups, study group one had 149 patients and study group two had 100 patients. Study group one received Ofirmev and study group two did not. Group one had a mean age of 49, was 27% male, 52% bariatric surgery, 12% abdominal surgery, 12% orthopedic surgery, and 13% other surgery. Group two had a mean age of 58, was 30% male, 48% bariatric surgery,11% abdominal surgery, 11 orthopedic surgery, and 13% other surgery. The statistical difference was in age between the groups.
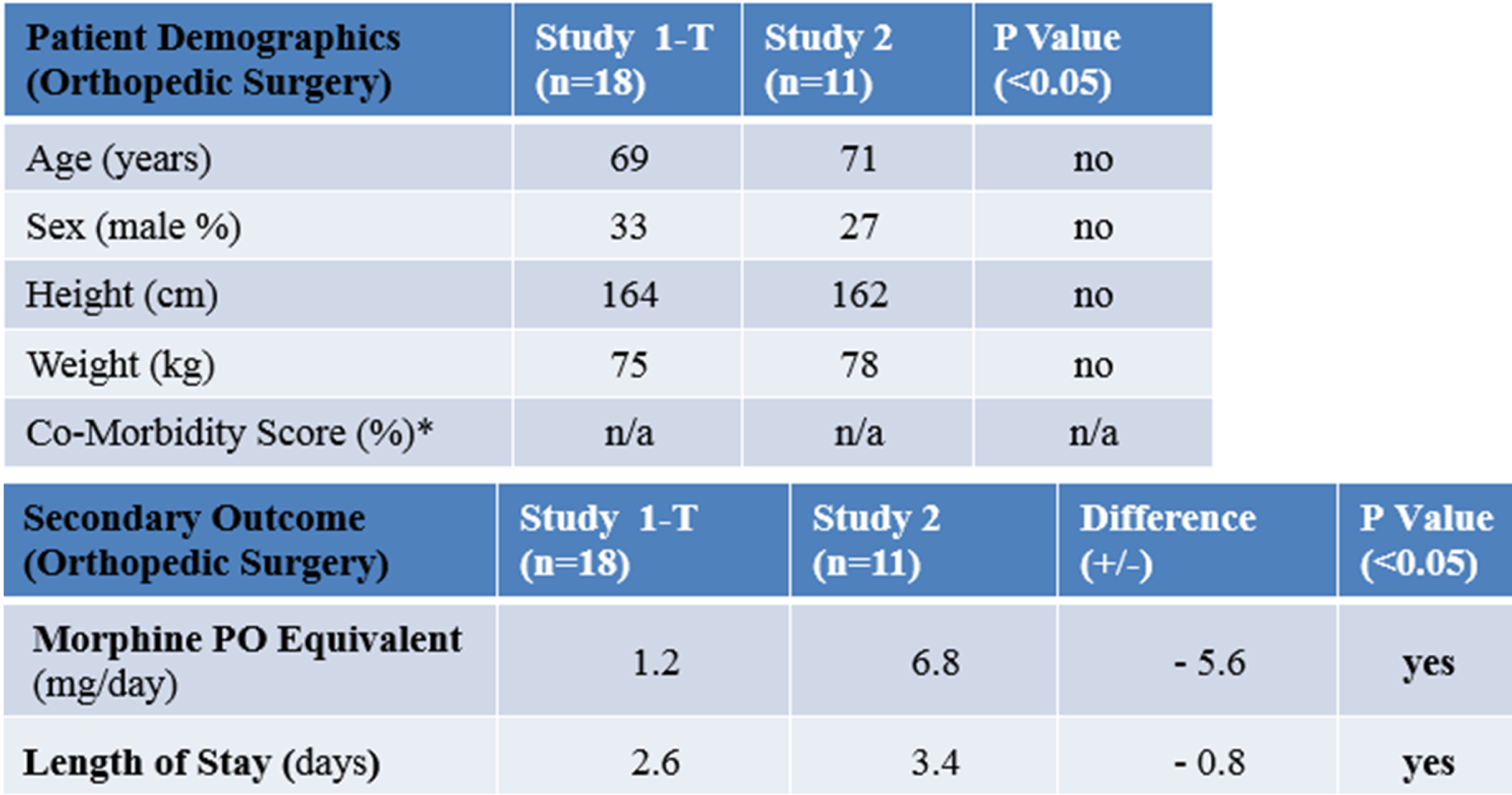
Of those orthopedic patients, group one (Ofirmev group) received 5.6 mg of morphine less a day and had an LOS of 0.8 days less which was statistically significant. A secondary outcome was in the bariatric surgery group, in group one with NSAIDs received 3.5 mg less of morphine a day and the LOS was 0.2 days longer.
Conclusions: Intravenous acetaminophen was not associated with a clinical or statistically significant difference in mean LOS, or reduced opioid requirements in all surgeries that would offset the additional cost. IV acetaminophen was associated with a clinical and statistically significant difference in mean LOS and reduced opioid requirement in orthopedic surgery offsetting the additional cost. Comparing the use of acetaminophen alone or in combination with NSAIDs for postoperative pain in bariatric surgery, it showed that the combination was no more effective than Ofirmev alone and resulted in a statistically significant but nonclinical increase in LOS.