
Background: Perioperative management of anticoagulant in mechanical valve patients is challenging, Current recommendations focus on management in patients undergoing elective surgery, while the data in patients hospitalized for emergency/urgency non-cardiac surgery is limited. We aimed to identify thromboembolic and bleeding events after anticoagulant interruption in patients with mechanical heart valves hospitalized for emergency/urgent non-cardiac surgery. Also, we expected to find out a proper duration of anticoagulant interruption in these patients.
Methods: We extensively reviewed data of hospitalized patients with mechanical heart valve whose warfarin were interrupted for emergency/urgency non-cardiac surgery or intervention during January 2010 to July 2015 in a teaching hospital. All demographic data, history of prostatic valve replacement, perioperative anticoagulant management, duration of anticoagulant interruption and outcomes of these patients were collected and then were analyzed.
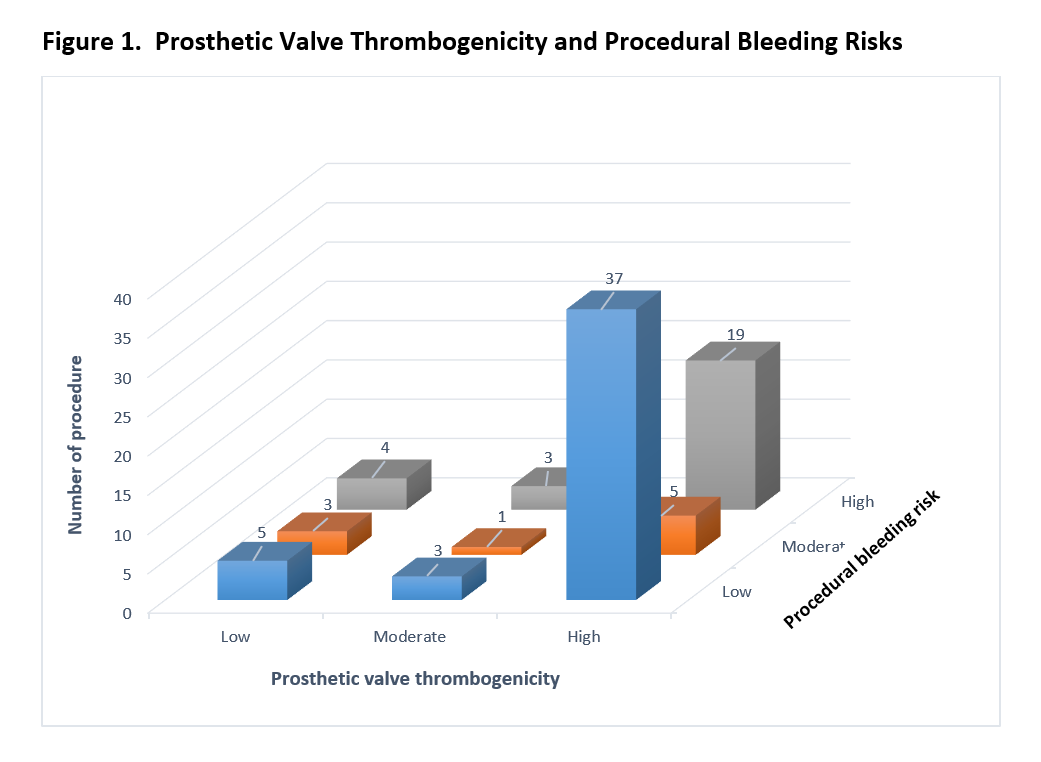
Results: From 1,079 hospital admissions of prosthetic-valve patients, there were 59 admissions, 55 patients with 80 procedures, met our criteria (unexpected surgical procedure or intervention that should be done within 48 hours since the patients were admitted). Twenty-three (41.8%) were male and the mean age was 58.9 years. Among 55 patients, prosthetic valve thrombogenicity were classified as high in 44 (80%), moderate in 5 (9%), and low in 6 (11%) patients according to international guidelines. The risks of bleeding were considered as high in 26 (32.5%), moderate in 9 (11.25%) and low in 45 (56.5%) procedures as shown in figure 1. Warfarin therapy was interrupted in all patients with a median interruption time of 3 (2,6) days and the longest duration of anticoagulant interruption was 15 days. One patient (1.8%) developed valve thrombosis, one patient (1.8%) with atrial fibrillation had subsequent systemic embolism, and 6 (10.9 %) patients had clinically significant bleeding within 30 days after the procedure. Among patients without adverse event, the median duration of anticoagulant interruption times was 6 (3,7) in patients underwent high -bleeding risk procedures. and 3.5 (1,5) in patients underwent low-bleeding risk procedure. (Table 1)
Conclusions: Optimal management of patients with prosthetic valve hospitalized for Emergency/Urgency Non-Cardiac Surgery has not yet been established resulting in high morbidity and mortality by current practices. Further study among this patient group should be conducted.
.png)