Background: Consensus supports the use of corticosteroids in acute exacerbation of COPD (AECOPD), but route of administration and dosage still vary considerably. In one study comparing lower dose oral (PO) prednisone to higher dose intravenous (IV) methylprednisolone, the prednisone regimen was associated with comparable improvement in lung function and oxygenation but a trend toward significantly fewer adverse events related to hypertension and hyperglycemia. Furthermore, another study demonstrated lower treatment failure rates, length of stay and direct costs in patients treated with oral corticosteroids. We propose that the use of intravenous route of administration results in inadvertantly higher corticosteroid dosing for AECOPD hospitalizations.
Methods: A retrospective chart review was performed of patients admitted for AECOPD to a 552-bed academic tertiary care medical center between September 2012 and May 2014. AECOPD hospitalizations were identified by ICD-9 billing codes. Exclusion criteria included patients who left against medical device, were admitted/transferred to ICU level care, or upon further chart review were thought not to be experiencing AECOPD by reviewers. All corticosteroid doses were converted to prednisone equivalent, and patients receiving IV corticosteroids were compared to those receiving oral route of administration
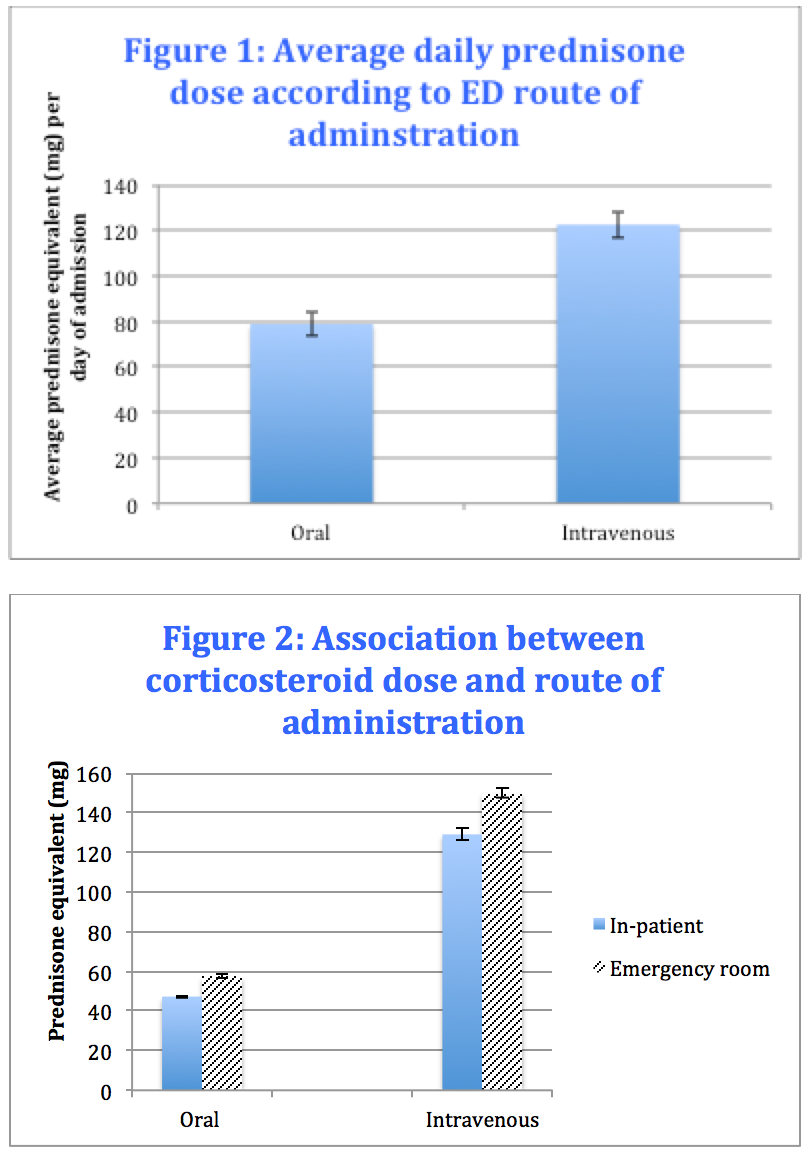
Results: Over the 20-month period, AECOPD hospitalizations were identified by ICD-9 billing codes. 314 patients were analyzed after exclusion criteria were applied. 46% (n=146) received IV methylprednisolone (MP) versus 34% (n=107) receiving oral prednisone in the ED. The mean IV dose was 129.1 mg of prednisone equivalent for inpatients and 149.8 mg in the ED while oral doses were 47.3 mg for inpatients and 57.2 mg in the ED (Figure 1). IV administration of corticosteroids in the ED was associated with a dose of 122.6 mg of prednisone equivalent per day while PO administration was associated with 78.9 mg of prednisone equivalent per day during inpatient hospitalization (Figure 2).
Conclusions: Our results demonstrate an association between IV route of administration and higher steroid burden, and this association is strong even when only considering the first dose administered in the ED. To address unnecessarily high corticosteroid dosing in AECOPD, we propose interventions that lead to lower doses that are more consistent with current treatment guidelines for non-ICU AECOPD hospitalizations. These will include changing the default corticosteroid dosage in an electronic medical record COPD order set to lower dose oral, adding a formula to convert oral prednisone to IV route, and advising providers to consider switching to lower oral doses in patients started on higher IV doses.