Background:
Transitions from hospitals to the ambulatory setting are high risk periods for patients. The advent of the Patient-Centered Medical Home (PCMH) and Accountable Care Organizations (ACOs) provide an opportunity for true collaboration in which both inpatient and outpatient providers contribute to improving transitions in care. The goal of this study was to develop, implement, refine, and evaluate a multi-faceted, multi-disciplinary transitions intervention across two hospitals and 18 PCMHs within a Pioneer ACO.
Methods:
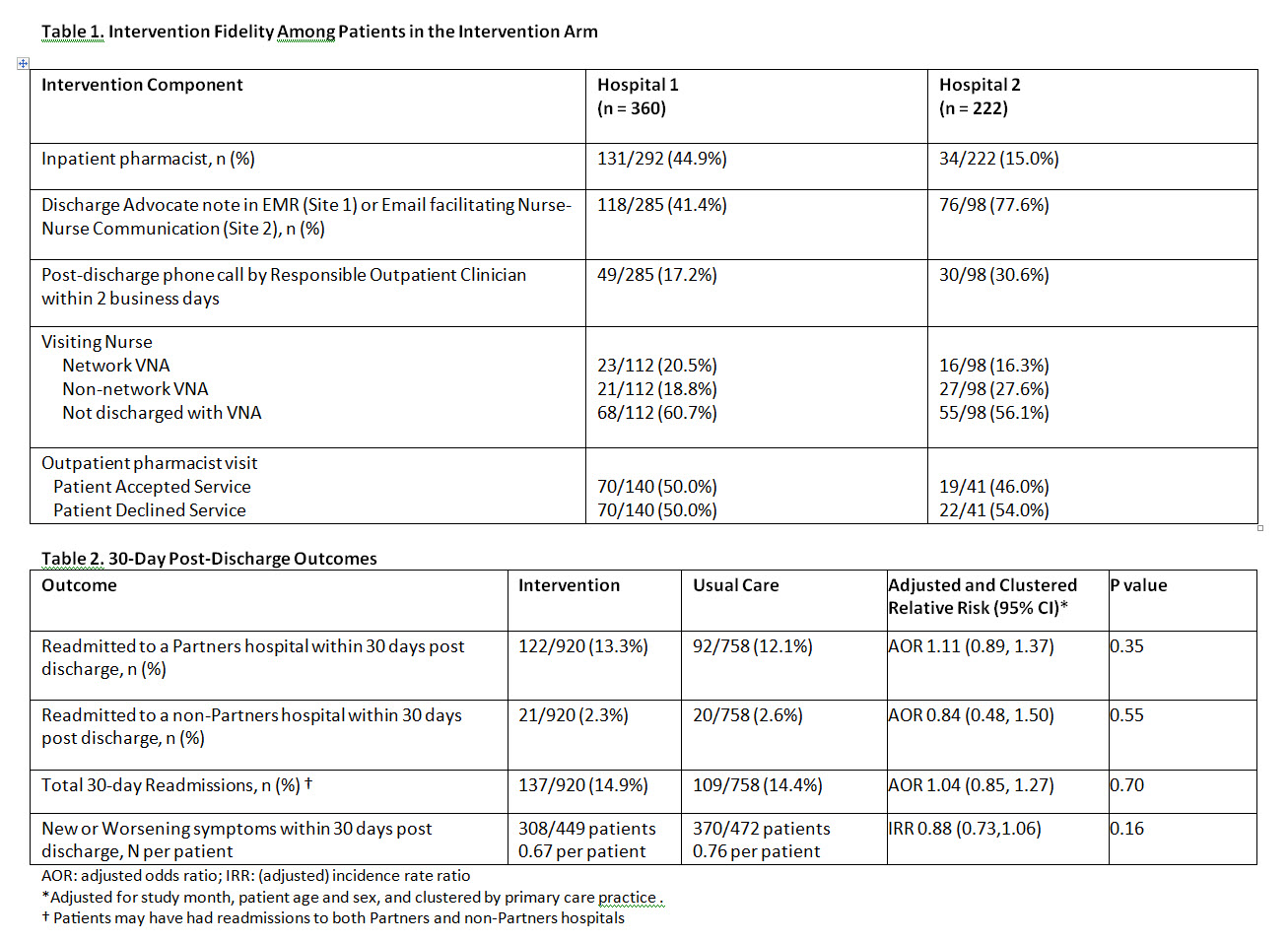
We developed an intervention with the following components: inpatient pharmacist-led medication reconciliation and patient counseling; coordination of care and patient education from an inpatient Discharge Advocate and PCMH Responsible Outpatient Clinician; a structured visiting nurse intervention; structured post-discharge phone calls; timely follow-up visits; tools to improve communication among care team members; and home pharmacist visits for selected patients. The study used a “stepped wedge” design in which each PCMH practice started in the usual care arm and then at a randomly selected point in time changed to the intervention. Outcomes included 30-day hospital readmissions using medical records and telephone follow-up; and new or worsening symptoms in the 30 days after discharge based on telephone follow-up. The two outcomes were analyzed by multivariable logistic and Poisson regression, respectively, adjusted for study month, patient age and sex, and clustered by primary care practice.
Results:
1678 patients were enrolled, including 758 assigned to usual care and 920 to the intervention. Receipt of different components of the intervention varied by component (Table 1) and in some cases by hospital, unit, and practice. 30-day readmission rates were 14.9% in the intervention arm and 14.4% in usual care (p=0.70; Table 2). The number of new or worsening symptoms was 0.67 per patient in the intervention arm and 0.76 per patient in usual care (p=0.16).
Conclusions:
Results showed no difference in 30-day readmission rates among patients in the two study arms, likely due to lower than expected intervention fidelity and the low proportion of readmissions that are truly preventable in this patient population. The intervention was associated with a non-significant trend towards reduced new or worsening symptoms in the post-discharge period, an outcome more sensitive to change than readmissions. As with readmissions, efficacy was likely limited by intervention fidelity. Further study is needed to further explore the causes and effects of low intervention fidelity, determine the most important components of the intervention, and determine patient subgroups most likely to benefit from these types of interventions.