
Background:
Hepatitis C virus (HCV) is the most frequent cause of chronic liver disease. Many patients suffering from prolonged HCV develop cirrhosis that may lead to decompensation events, such as hepatic encephalopathy (HE). Rifaximin (RFX), a minimally absorbed, gut‐targeted antibiotic, has demonstrated efficacy and safety in a heterogeneous group of cirrhotic patients with recurrent HE, although the profile in specific subgroups of patients has not been examined. The objective of this analysis was to assess the efficacy and tolerability of rifaximin in maintaining remission from HE in cirrhotic patients with HCV.
Methods:
Breakthrough HE events and tolerability were assessed from a 6‐month, randomized, double‐blind, placebo‐controlled trial of RFX 550 mg twice a day in cirrhotic patients (n = 299) with a recent history of recurrent HE but in remission at enrollment (Conn Score [CS], 0 or 1). Breakthrough overt HE was defined as an increase in CS to ≥2 or an increase in both CS and asterixis scores of 1 grade each for patients entering with a CS of 0. Lactulose was permitted throughout the study. The incidence of adverse events (AEs) was reported.
Results:
HCV was the etiology of advanced liver disease in 42.8% of patients (128 of 299). Demographic and baseline characteristics were generally similar between HCV and non‐HCV patients. In HCV patients, breakthrough HE events occurred in 26.2% of RFX patients (16 of 61) versus 47.8% of PBO patients (32 of 67), corresponding to relative reduction in risk of a breakthrough HE episode of 52.2% (P = 0.014; Figure). In cirrhotic patients with other etiologies (e.g., alcohol‐related, NAFLD/NASH), there were also significant treatment‐related differences, with 19.0% of RFX patients (15 of 79) experiencing a breakthrough HE event versus 44.6% of PBO patients (41 of 92) — P < 0.001. In HCV patients, the most commonly reported AEs were nausea (RFX, 18.0% of patients; PBO, 19.4% of patients), fatigue (RFX, 14.8%; PBO, 13.4%), and peripheral edema (RFX, 14.8%; PBO, 7.5%).
Conclusions:
In patients with HCV and recurrent HE, RFX was efficacious and well tolerated, with a clinical profile similar to that observed for cirrhotic patients with other etiologies of advanced liver disease.
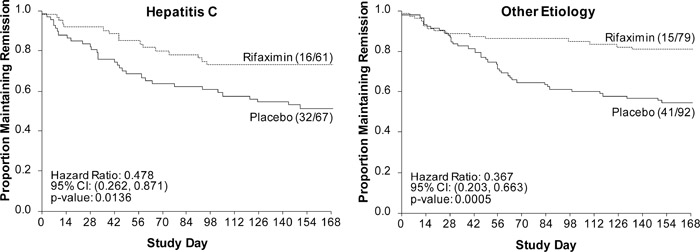
Hepatitis C versus other etiologies.