Background: Patient lists and patient assignment aid hospitalists through their workflow. Lack of a standardized approach has led to various ways of patient assignment and various means to display them. With the evolution of electronic medical records and technology; patient assignment and their display theoretically should have been more straight forward however there are still wide variations in how patients are assigned.
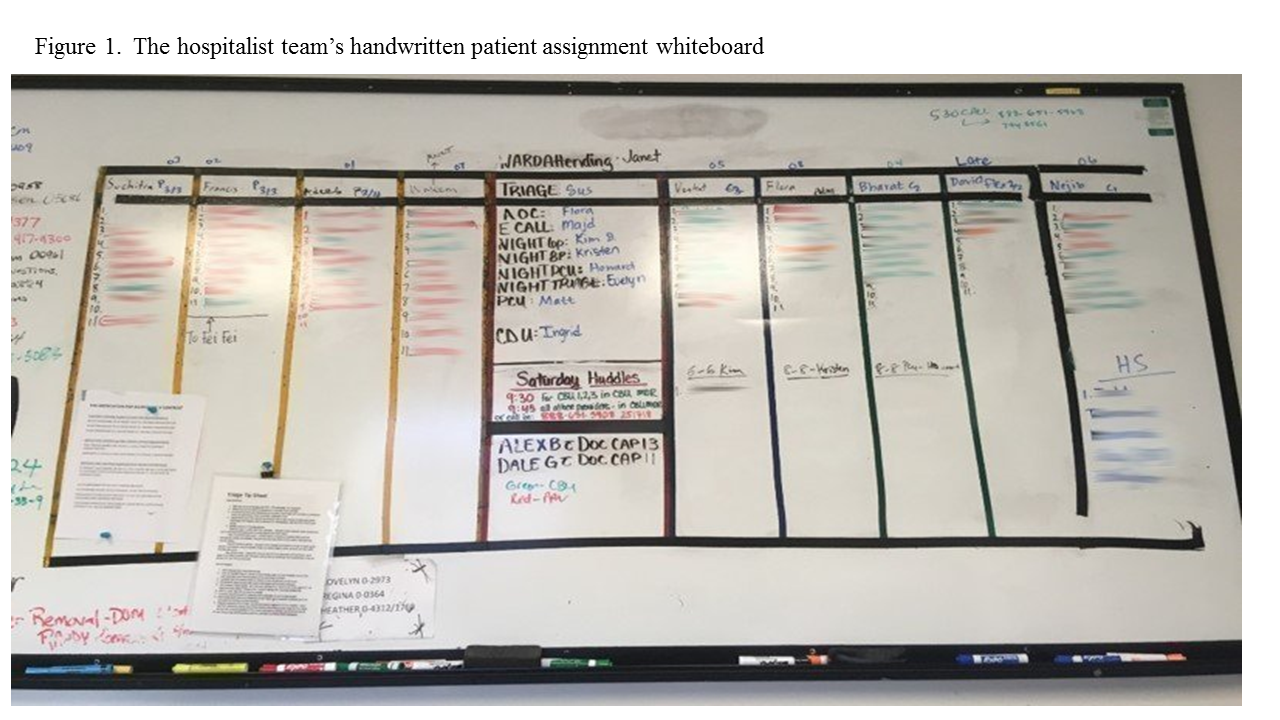
Purpose: Within our division we employed a hand written white board and manually assigned patients despite the advent of EPIC in 2015. A home grown “Signout” system helped track patient coverage and movement prior to EPIC. Post EPIC go live, the home grown system was phased out and EPIC took over its roles. However the tedious process of updating the board manually, workflows being centralized around the board and reliance on manually adding and removing patients meant redundant work and human errors. To decrease redundancy, human errors and embrace technology we embarked on a journey to make patient assignment electronic and display of assignments electronic.
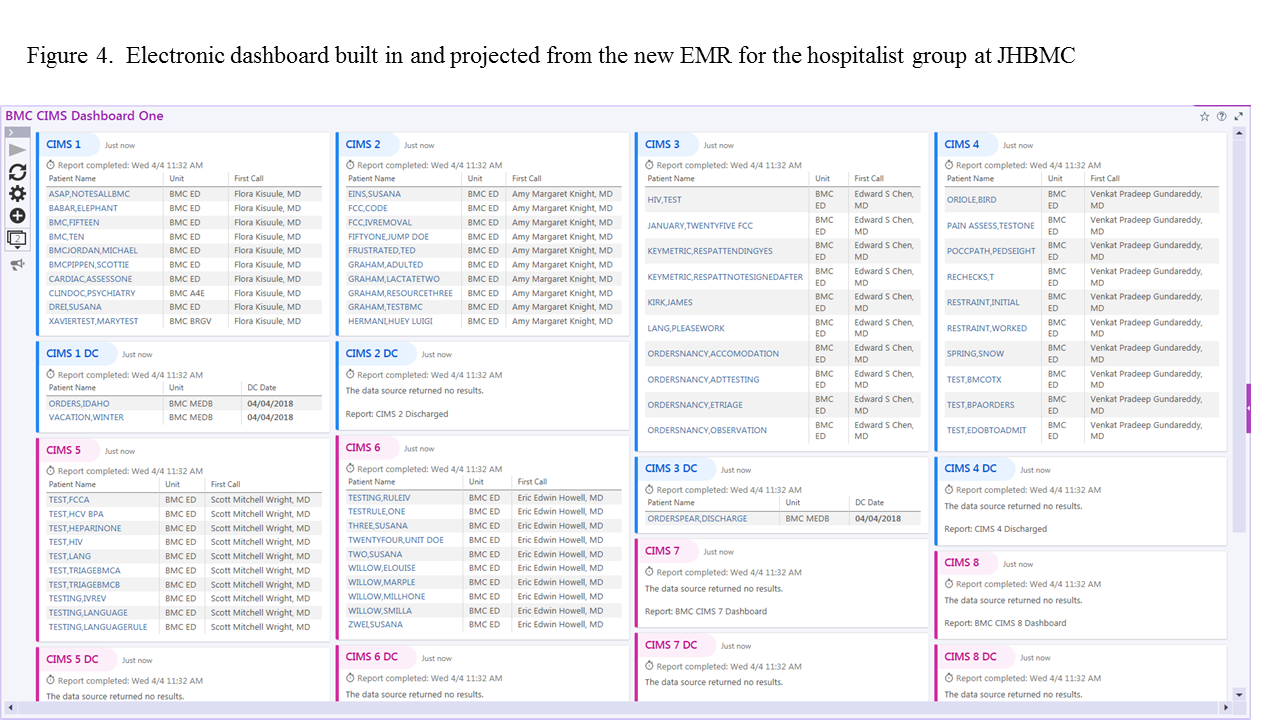
Description: With collaboration with EPIC Team, we were able to create a radar dashboard that would mimic the display on the handwritten white board. This was capable of being displayed on a wall mounted monitor. To prepare for this transition and improve the efficiency with which patients were transferred from one provider to another, the group reorganized itself from one team into 10 distinct teams, CIMS 01 – CIMS 10. The team assignment for each provider working on a given day was noted in the proprietary scheduling system. Each new team had two new corresponding system lists built in Epic, one for active patients and one for patients discharged in the last 24 hours. Dashboard development relied on patient care teams and patient lists as the base build and the dashboard was configured as follows: Each new team was given two Dashboard Components (“widgets”), one for active patients and one for recently discharged patients. Widgets are lined up four across, and each row of active and discharged patient widgets has the same color to improve the visual cohesiveness. Each row in an active and discharged patient widget displays a patient’s last and first name, unit, and the name of their First Call Provider. The Dashboard was then “automated” using a batch process, eliminating the need to manually run the report each time the physician needed to see the most current patient status.
The Radar dashboard was ready for desktop use before the configuration was ready for display on the wall-mounted monitor. After a multi-team collaboration between the Epic Orders, Database Admin and Sr. LAN Admin Teams, the wall monitor went live, the dashboard display was presented, and team members were told to stop recording patient assignments manually and rely exclusively on the dashboard.
Newly admitted patients are continuously added to the dashboard. Patients who are discharged are left on the list until the end of the day providers’ shift to ensure that they are considered when determining whether a provider has reached his or her “cap”, or has the capacity to take a new admission.
Conclusions: Patient assignment is a daily occurrence in every hospitalist service. Integrating technology with human effort would lead to a less redundant more efficient systems that would have patient and provider benefits; as was in our case. We envision a future patient assignment dashboard that is algorithm based and incorporates patient continuity, acuity, discharge predictors and geographic cohorting.