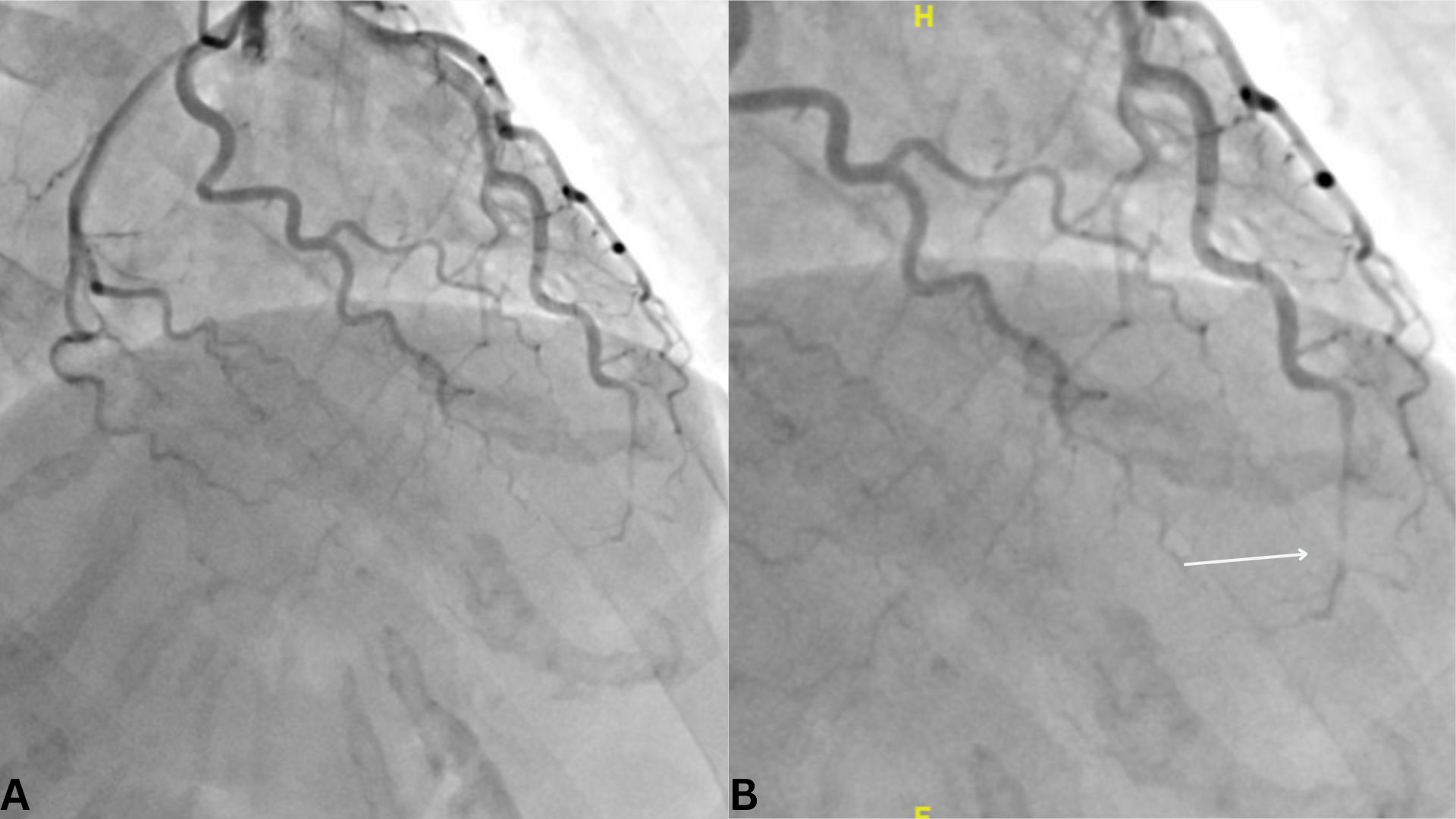
Case Presentation: A 56-year-old post-menopausal female with no prior medical history presented to the ED with two days of substernal chest pain radiating to the left shoulder, worsened 1-2 hours prior, and associated with fatigue. Two days earlier, she experienced significant emotional stress during a custody-related phone call, during which her husband observed her becoming flushed and trembling. Her usual systolic BP was < 110 mmHg, but she recorded 135 mmHg after the event. She denied systemic symptoms, smoking, or alcohol use. Family history included a grandfather with myocardial infarction at 77.In the ED, BP was 160/106 mmHg, and high-sensitivity troponin was elevated at 255 ng/L (normal: < 19 ng/L). ECG showed ST-segment elevation in leads II, III, aVF, V3, and V4, with ST depression and T-wave inversion in lead aVL. Coronary angiography revealed SCAD of the distal LAD with TIMI-2 flow and no CAD (Figure 1). Echocardiogram showed LVEF of 40-45% with apical hypokinesis and aneurysm. She was treated with DAPT, losartan, metoprolol, and atorvastatin, with symptom improvement and LVEF recovery to 52% on follow-up.
Discussion: Spontaneous coronary artery dissection (SCAD) is a rare cardiovascular condition where the artery dissects between the intima and media layers or forms an intramural hematoma due to leakage from the vasa vasorum [1]. It often mimics myocardial infarction with chest pain, ST-segment elevation, and palpitations but does not involve atherosclerotic blockage [2]. SCAD is associated with fibromuscular dysplasia (present in 61% of patients), Marfan syndrome, Ehlers-Danlos syndrome, hypertension, and pregnancy [3,4]. Physical and emotional stress are recognized triggers, though cases in patients without risk factors are rare [5,6]. This case describes a 56-year-old post-menopausal female with no medical history who presented with SCAD following an emotional stressor, highlighting the potential role of stress and reduced estrogen levels during menopause in its pathogenesis.SCAD pathophysiology may involve catecholamine surges causing vasoconstriction and vessel shear stress, similar to Takotsubo cardiomyopathy but with coronary artery involvement [7]. Menopausal estrogen reduction compromises vascular integrity, increasing susceptibility to SCAD [8]. Diagnosis typically relies on coronary angiography; in uncertain cases, Optical Coherence Tomography (OCT) may aid visualization [9]. Conservative management with dual antiplatelet therapy, beta-blockers, and statins is recommended for hemodynamically stable patients [10]. Regular follow-up and cardiac rehabilitation are crucial due to risks of recurrent SCAD or complications like myocardial infarction or arrhythmias [11].This case highlights the importance of recognizing rare cardiovascular conditions in acute care settings. While SCAD often mimics myocardial infarction, careful attention to patient demographics and clinical context, such as emotional stress or hormonal changes, can lead to an accurate diagnosis and appropriate management. This case emphasizes the value of hospital-based frameworks in refining diagnostic approaches and facilitating coordination with specialty teams for complex cases encountered during hospital admissions.
Conclusions: SCAD diagnosis in atypical patients challenges hospitalists to refine inpatient strategies. Understanding stress, hormonal shifts, and vascular health is crucial for timely interventions and optimizing inpatient outcomes.