Background: Murine typhus, a flea-borne rickettsial disease traditionally found in warm, humid climates, is increasingly reported in non-endemic regions due to factors such as climate change and urbanization. Characterized by nonspecific symptoms including fever, headache, rash, and elevated liver enzymes, murine typhus often mimics common febrile illnesses such as influenza, viral exanthems, or sepsis. Delays in diagnosis can result in prolonged hospital stays, unnecessary diagnostic tests, and inappropriate use of broad-spectrum antibiotics. Hospitalists, as the first point of contact for hospitalized patients, are uniquely positioned to identify murine typhus early, reducing the need for infectious disease (ID) consults and expediting appropriate care.
Methods: The electronic medical record system was used for retrospective analysis of patients charts for patients within the Harris Health System. 79 charts were between 01/30/2019 – 01/30/2024 found to have (+) Murine Typhus IgM and/or IgG. 7 patients were excluded if they were outpatient, had an incomplete chart to review, were diagnosed and cared for outside of Harris Health, had too low of titers to make the diagnosis, or diagnosis was not consistent with murine typhus. Demographics, clinic and admission dates, length of stay, comorbidities and medications, animal exposures, symptoms, vitals, physical exams, labs, imaging, treatment course, illness complications, timing and antibiotic selection, whether infectious disease was consulted, and fever clearance time was documented.
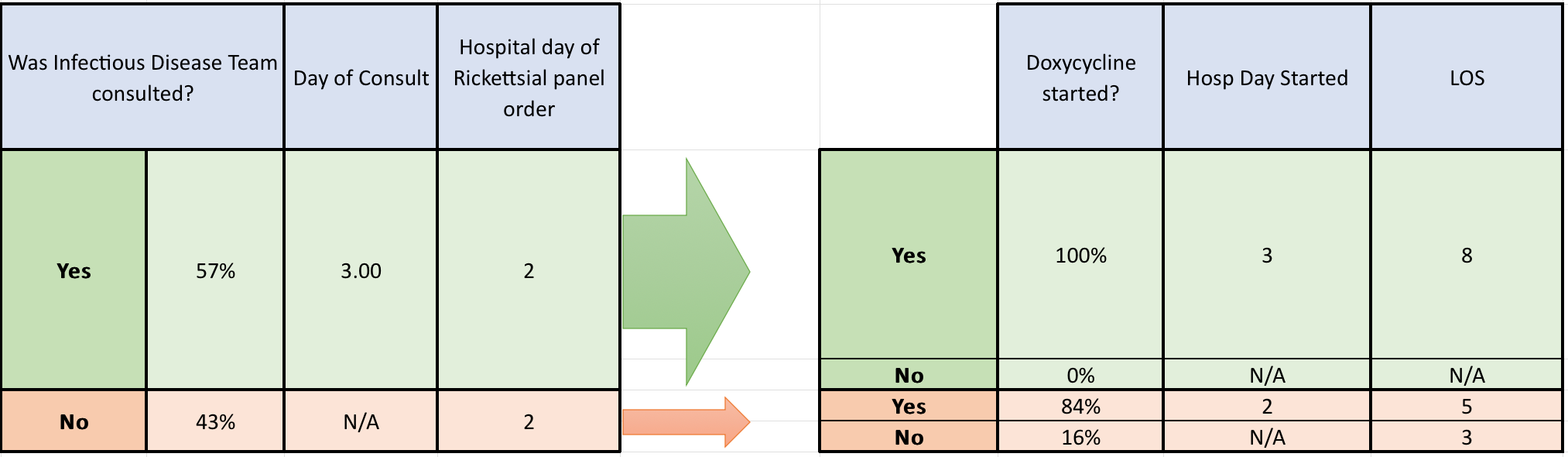
Results: 73 patients with murine typhus were identified. Mean age 43.8, 59% males, 41% females. Most common presenting features were fever (72%), headache (53%), myalgias (51%), rash (48%), thrombocytopenia (68%), and elevated liver enzymes ALT (75%) and AST (89%). LFTs were elevated in a hepatocellular injury pattern with predominance of ALT and AST elevated. Mean total bilirubin elevation 1.5. Mean alkaline phosphatase 141.6. Peak WBC count 11.2, while 100% of patients met criteria for sepsis on vitals. 33.9% had splenomegaly, 62.7% had hepatomegaly on CT imaging. Infectious Disease team was consulted 57% of the time with an average day of consult on day 3 and Infectious Disease team consulted resulted in doxycycline being started 100% of the time. Doxycycline was only started 84% of the time when ID was not consulted. The average time until last fever after starting antibiotics was 52.65 hours. In some cases fevers cleared prior to doxycycline starting.
Conclusions: Hospitalists play a pivotal role in recognizing murine typhus early, particularly in regions with expanding endemicity. Empowering hospitalists with a clinical framework for suspecting and diagnosing murine typhus can reduce delays in care, improve outcomes, and optimize antimicrobial stewardship. Recognizing a pattern of most common presentation symptoms, lab findings, imaging findings, and fever curve for murine typhus is important for all hospitalists. Education and dissemination of this framework can help reduce reliance on ID consults, ensuring timely, targeted therapy in affected patients.