Background: Large hospital systems receiving transfer from other facilities constantly experience bed shortage and need to have real time awareness of all its’ facilities capacity, capability, and services currently available. Our hospital system receives about 150 inter-hospital transfer requests daily and complete about 60 each day. We have a centralized transfer center where our Transfer Coordinators (TC) with nursing background, previously handled all medical complexities and nuances that involve each transfer request, presenting a huge clinical challenge to them.
Purpose: To address this problem, we created Transfer Center Physician (TCP), a dedicated position that offers clinical and administrative oversight for all adult transfers, initially 7am to 7pm, Monday to Friday. Previously all transfers queries were assigned to a provider who also had rounding responsibilities. Due to high transfer volumes, this led to delays in calling back to the Transfer Center and provider burnout. As of October 2024, the TCP position has been in operation for one year, and we tracked several metrics to assess what are the benefits of a TCP.
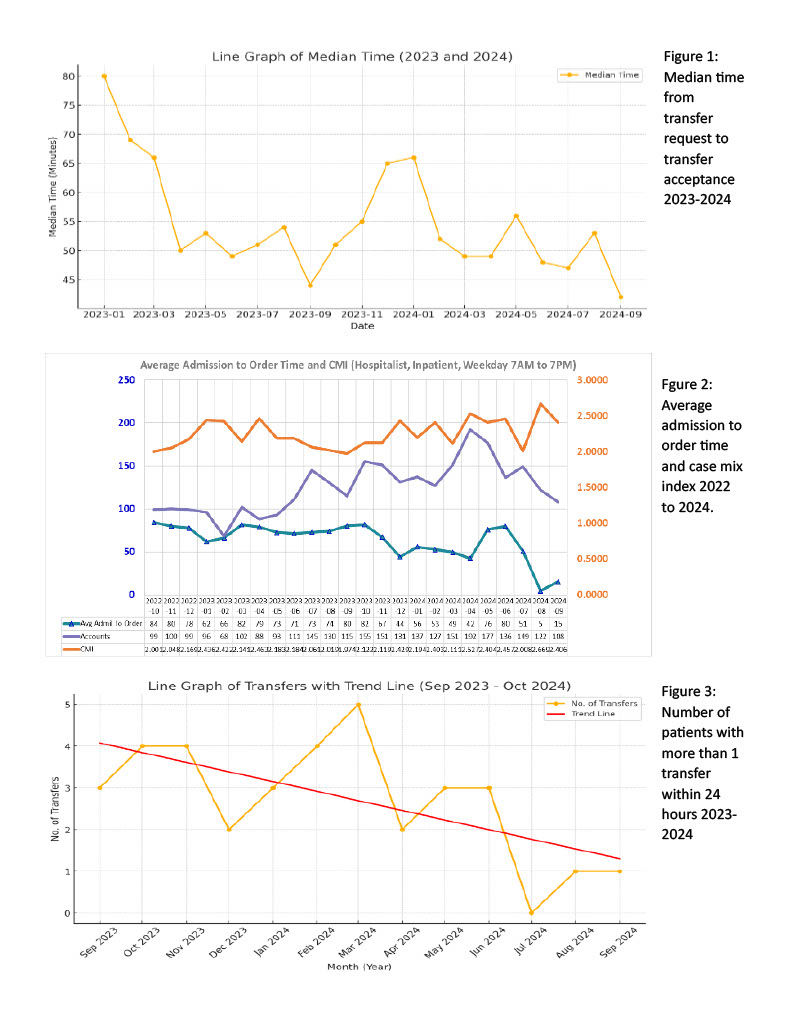
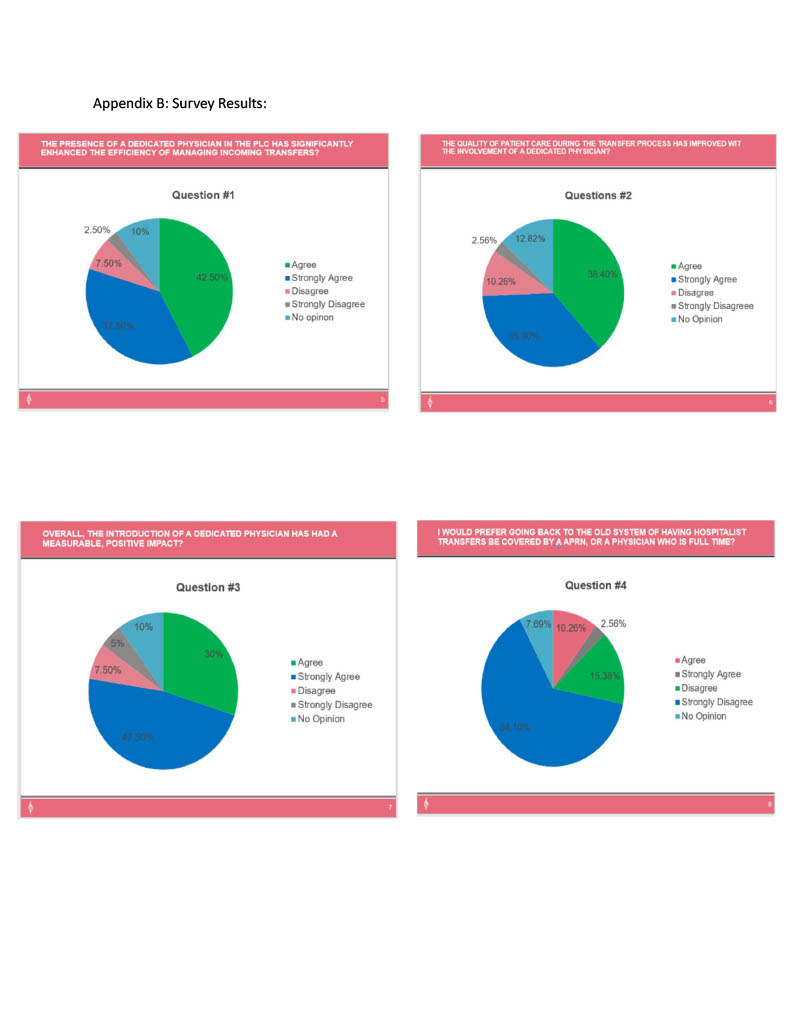
Description: We tracked about 10 different metrics which included (1) time from transfer request to acceptance, (2) case mix index (CMI), (3) admit to order placed time (4) patients with more than one transfer within 24 hours and (5) provider satisfaction. Regarding the time taken from request to acceptance, our benchmark was under 60 minutes. By having a TCP, we noted our monthly median time consistently stays below 60 minutes for most months (Figure 1), correlating to improved efficiency in reducing request backlogs. Looking at CMI, we recorded the single highest monthly average ever of 2.66 (Figure 2). Additionally comparing the last 6 months to the 6 months prior to initiating this position, our CMI increased from 2.069 to 2.4. This is an indication that we were weeding out unnecessary transfers and consistently placing the right patients within our facilities. The increase in CMI potentially lead to an increase in revenue of over $2,000 per case. Our admission to order time reduced with the aid of a transfer center admission order set developed by the TCP, whereby the TCP could now place admitting orders ahead of patient arriving (Figure 3). Routine orders such as vitals, labs, diet or pain medication were placed ahead of patient arrival, reducing calls to admitting physicians and minimizing delay of care of patient. Looking at the appropriateness of transfer, we noted a decline in the number of patients who had more than 1 transfer within 24 hours (Figure 3), which is an expensive event. We noted months when no double transfer within 24 hours were recorded. Lastly, from a workforce experience perspective, we conducted a survey of TCs and hospitalist staff on whether TCP position improved their workday experience, with approximately 80% of responders agreeing that it did. (Appendix B).
Conclusions: Within one year of having a TCP, the promise of this role has led to the approval of additional staff, now allowing year-round 7am to 7pm TCP role coverage. With the added manpower, we now are drilling further down to tackle constraints during patient transfer. We have better rapport between the transfer center and other hospital staff that has led to more innovations such as development of validated clinical guidelines that guide transfer of specific conditions such as compression fractures, inpatient chemotherapy, or intervention radiology procedure. All this will depend on and benefit by having a dedicated TCP.