Background: Hospital at Home (HaH) is an expanding clinical model that delivers inpatient-level care to patients in their homes, substituting a traditional hospital stay. It is becoming a standard of care at many institutions, yet there are still few formally established processes for integrating medical trainees despite clear benefits for both the program’s growth and the trainees’ educational experience. Participation in HaH offers trainees a unique opportunity to gain hands-on experience in delivering acute home-based care, navigating the challenges of telemedicine, and collaborating with a decentralized, interdisciplinary team. Involving trainees has the potential to significantly enhance the dissemination of information about the HaH model within the inpatient setting, ultimately leading to an increase in patient referrals. Exposure to HaH during training will also help ensure the growth and sustainability of the HaH provider workforce, who will continue to drive program innovation
Purpose: Our aim was to create and implement a formal HaH curriculum for internal medicine residents within our health system.
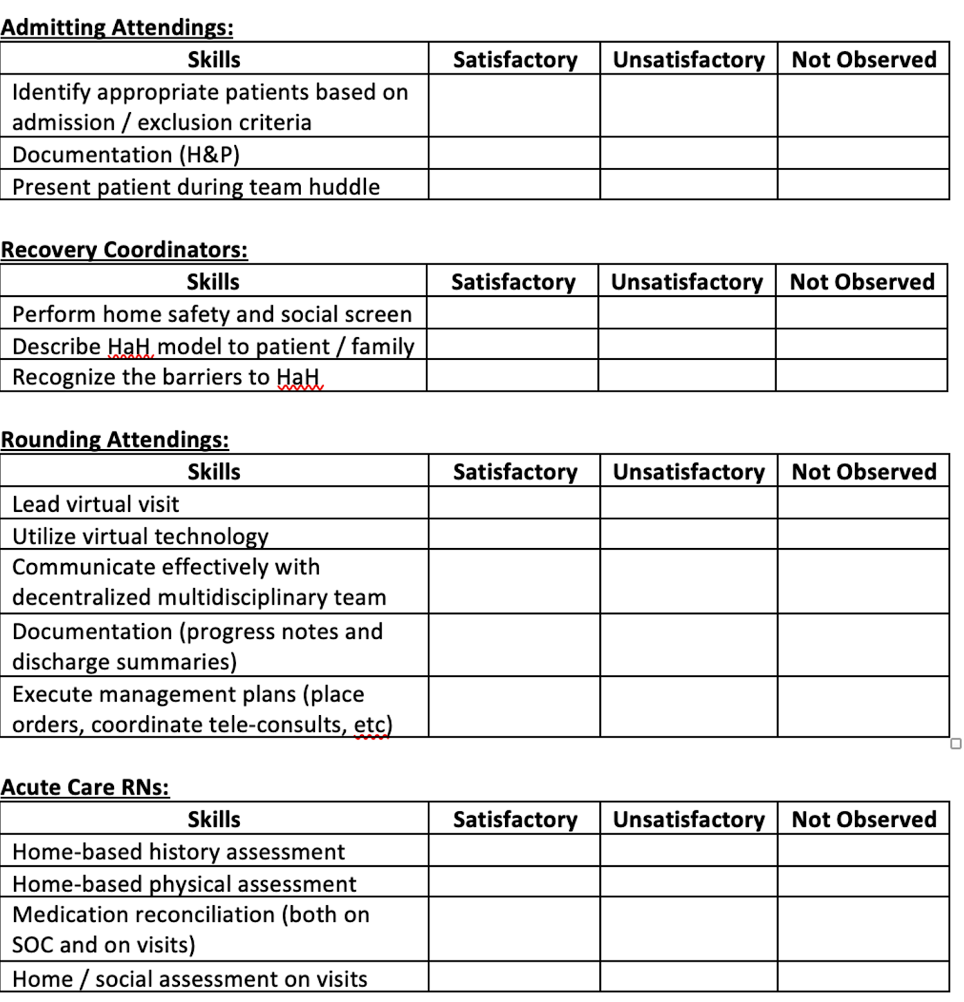
Description: A standardized HaH curriculum was developed for internal medicine trainees across all postgraduate levels and implemented in July 2024. The structured daily framework ensures that trainees actively participate in all aspects of the program, including patient screening, admitting, virtual rounding, and home visits. Trainees care for patients in the HaH model as they would on the wards, under direct attending supervision, and receive regular feedback to facilitate continued learning. They collaborate with nursing to perform in-home rounding and work with the acquisition nurse to learn the admission process. They also coordinate patient care with decentralized clinical and administrative teams. Trainees’ learning is supplemented by a lecture series led by members of the leadership team. A web-based tool provides further educational materials, including instructions and expectations for the rotation, as well as references to seminal HaH literature. Trainees are evaluated through direct observation of specific skill sets by the core HaH staff (Table 1). Pre- and post-elective surveys are administered to assess residents’ knowledge of the HaH model and their comfort level with HaH referrals gained through completion of the elective. Information about the elective was disseminated to the residents through large group teaching sessions, with the support of residency leadership. Since the implementation of the formal curriculum, enrollment has increased from 7 residents in the 2023 – 2024 academic year to 9 residents thus far from July to November 2024. An additional 7 residents are already registered for the elective between December 2024 and June 2025.
Conclusions: We successfully developed and integrated an educational residency curriculum into our HaH model, incorporating both virtual and in-person components. Feedback from trainees has been overwhelmingly positive. Trainee involvement has also been well perceived by our staff and patients and has helped introduce innovative perspectives to our currently established protocols. Data from pre- and post-elective surveys is being analyzed to implement curriculum changes. We plan to continue to expand the curriculum by incorporating additional educational sessions to enhance trainees’ understanding of the HaH care delivery model and its growing relevance in the current healthcare setting.