Background: Clinical reasoning errors are common, costly, and dangerous, yet difficult to study. Care transitions and the patient handoff offer opportunities to review and reassess care as well as provide valuable comparative feedback to clinicians. One educational area of improving clinical reasoning focuses on using multiple methods of feedback and reflection to learn from decisions and calibrate medical decision making (1-3). However, often in medicine, and particularly Internal Medicine night float rotations, residents admit many patients without feedback or awareness on subsequent diagnostic and management changes and outcomes (4-6). Programs targeted towards addressing this gap and understanding rates of diagnostic error in this population are rare, often focus on peer or self-level feedback, or limited by utilizing self-selected cases to review which are prone to selection bias (2, 6-9).
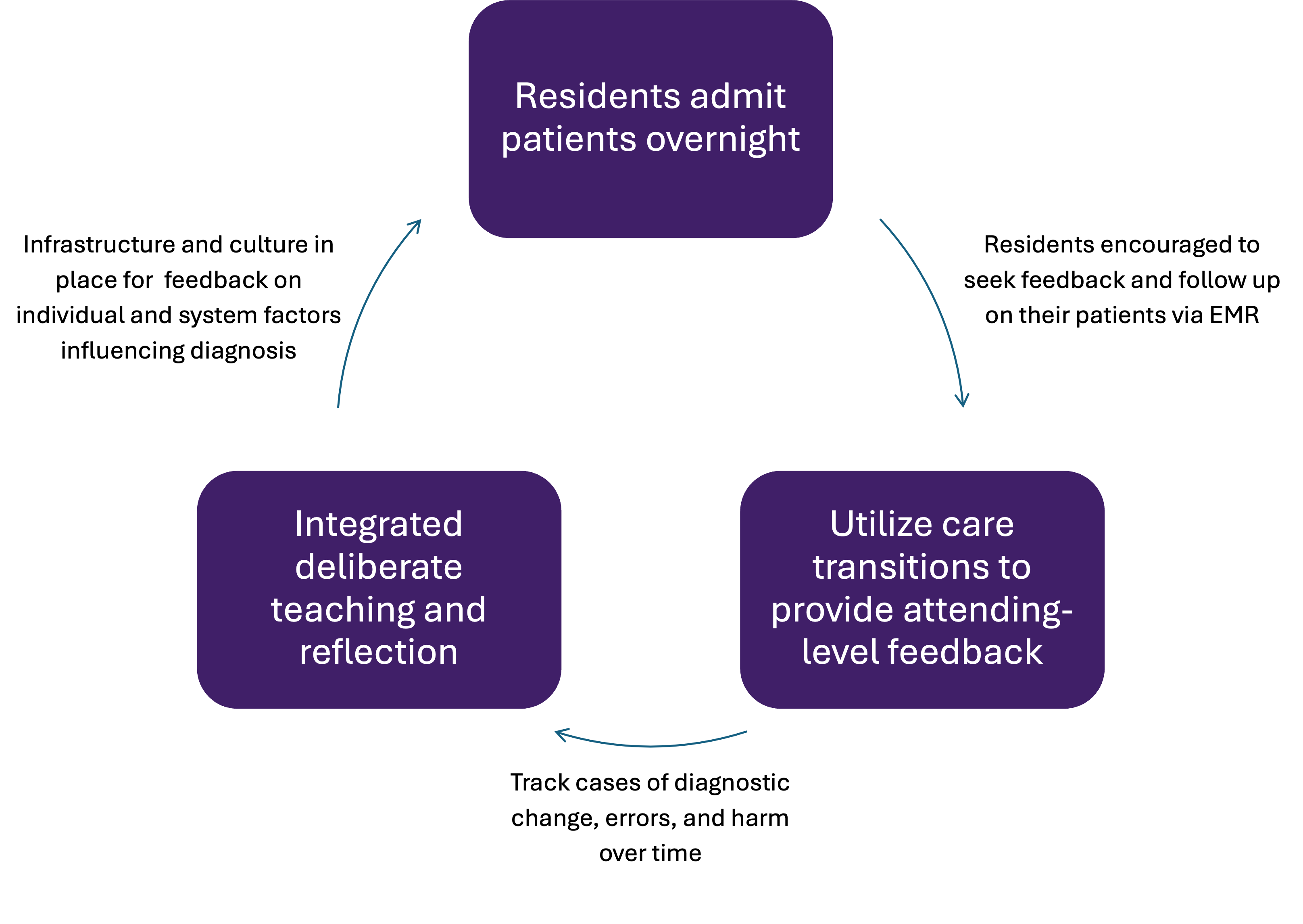
Purpose: We aimed to leverage care transitions to 1) study rates of diagnostic change, error, and harm in overnight internal medicine resident admissions; 2) provide attending-level feedback to residents on diagnostics and management; and 3) develop targeted opportunities for resident-driven deliberate reflection on clinical reasoning
Description: In this single-center study from Feb 2024 – May 2025 at a large academic Internal Medicine residency program, attending physicians on teaching services were sent questionnaires on a random subset of patients admitted overnight assigned to their team. Attendings noted changes in primary diagnosis, reasons for changes, and feedback on reasoning and management. Every 4 weeks, this attending feedback was sent directly to the admitting residents. Cases involving a diagnostic change were independently reviewed by 2 attending physicians. Cases were classified as diagnostic error and/or harm using published instruments (10) and categories of diagnostic process breakdowns were identified. Separately, night float residents completed end-of-rotation surveys, reflecting on clinical reasoning and admitting experiences. Periodic deliberate reflection sessions based on attending feedback and self-reflections have recently launched.
Conclusions: 127 of 207 (61%) questionnaires were completed by teaching attendings. 24 (19%) noted a diagnostic change, 14 (11%) involved a diagnostic error, and 2 (2%) were associated with harm. Common causes for error were missed history or information from electronic health record or failure to consider the diagnosis. These rates of diagnostic changes and error were lower than prior studies done in the night float resident population (6,7) – one possible reason being that this study used random cases rather than selecting cases by resident- or attending-choice or escalation of care situations. 26/70 (37%) residents completed the post-rotation survey, reporting high interest in this feedback with requests for more frequent and timely feedback. Data on deliberate reflection sessions were not collected. Overall, diagnostic changes and errors are common in night float medicine admissions – randomized analysis, structured feedback, and deliberate reflection provide opportunities for understanding the diagnostic error landscape in this setting and for providing clinical calibration opportunities to improve diagnosis.