Background: Excessive daily routine laboratory testing for hospitalized patients is a contributor to poor hospital sleep, iatrogenic anemia, and excessive costs. Recommendations from the Choosing Wisely™ campaign specifically state to avoid sleep interruptions for routine care (American Academy of Nursing) and to avoid routine labs for stable patients (Society of Hospital Medicine). The purpose of this resident-led initiative was to reduce indefinitely recurring daily labs in clinically stable patients and promote sleep-friendly ordering.
Methods: Using the COST (Culture, Oversight, Systems, Training) framework of value improvement, the Order S.M.A.R.T.T. (Sleep: Making Appropriate Reductions in Testing and Timing) campaign was launched at UChicago Medicine in March 2018. The committee included representatives from hospitalists, residents, nursing, lab medicine, informatics, and hospital leadership. A baseline survey assessed attitudes towards phlebotomy (Culture) and was used to inform the creation of a q48h 6AM phlebotomy option to “step down” from daily labs. We created two electronic medical record (System) interventions: 1) “Order Sleep” phlebotomy shortcut which provided 3 sleep-friendly options: 6 AM draw, 6 AM q48 hours draw, 10 PM draw and 2) A “4 AM Labs” icon on the patient lists to passively nudge providers that 4 AM labs were ordered. Training included lectures to Internal Medicine residents and Hospitalists. A single interrupted time series analysis was used to determine the changes in ordering practices (labs per patient per day) of sleep-friendly labs post-intervention while controlling for pre-intervention secular trends.
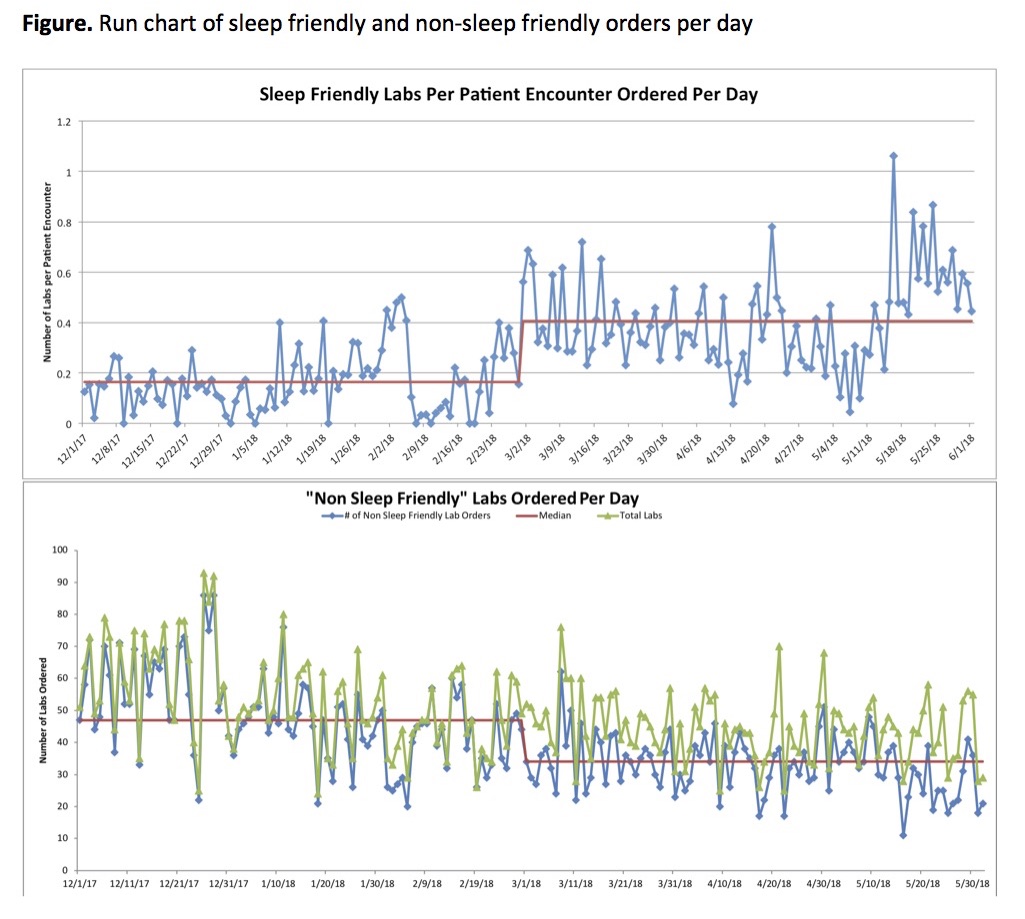
Results: Using a 6 month-time window, 27.3% sleep friendly labs per patient (n=488) were ordered pre-intervention compared to 67.2% post-intervention (n=1583). There was a significant increase in average sleep-friendly orders per patient encounter (0.164 vs. 0.406; p<0.0001) (Figure), with 23.9% sleep friendly labs per patient encounter pre-intervention versus 58.2% post-intervention. The single interrupted time series analysis demonstrated a significant increase of 0.148 in sleep-friendly orders per patient encounter per day immediately after the intervention (p=0.0014). Likewise, there was a significant decrease in the use of non-sleep friendly labs of .111 in non-sleep friendly lab orders per patient encounter per day immediately after the intervention (p=.0336). When examining total labs ordered, there was a significant decrease between mean value of total labs ordered per day between pre and post intervention (53.38 vs 44.31, p<0.0001).
Conclusions: An initiative using the COST value improvement framework can reduce daily labs while improving sleep-friendly ordering via an educational campaign and novel EMR tools on hospitalist and resident general medicine services.