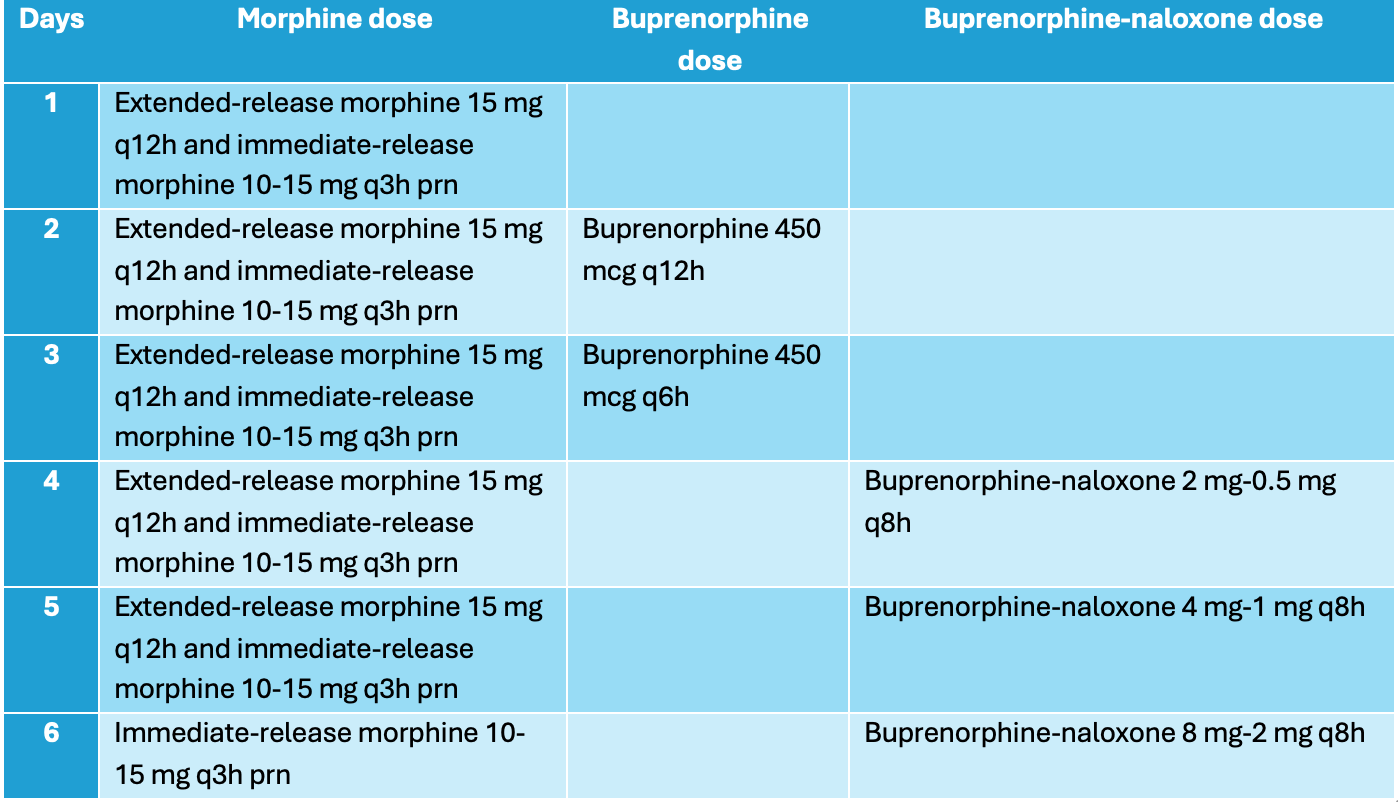
Case Presentation: A 59-year-old woman with a history of opioid use disorder (OUD), alcohol use disorder, heart failure, alcohol cirrhosis, and chronic kidney disease presented with right hip pain and was found to have right sacro-iliac joint septic arthritis with associated osteomyelitis and pelvic abscesses. She was started on as-needed IV hydromorphone, oral oxycodone, and scheduled acetaminophen. Throughout her hospital course, she underwent repeated abscess drainage procedures, with eventual drain placement. After multiple surgical interventions, our volunteer OUD consult team was contacted to assist as patient continued to have substantial pain and opioid cravings despite the above in-hospital regimen. Her opioid regimen was changed to scheduled oral extended-release morphine and oral immediate-release morphine as needed for moderate to severe pain (Table 1). Once her pain was well-controlled, a five-day low dose buprenorphine initiation (LDBI) was performed, overlapping oral-extended morphine with buprenorphine-naloxone (Table 1). Once the patient reached the goal buprenorphine-naloxone dose, extended-release morphine was discontinued, and her pain and cravings remained well-controlled. She was discharged with the above buprenorphine dose, and with referral to an outpatient addiction medicine clinic.
Discussion: Hospitalists are uniquely positioned to address OUD during hospitalization, when patients are often most receptive to treatment and closely monitored. There is limited literature documenting management of opioid cravings and acute-on-chronic pain with oral extended-release morphine, followed by LDBI in the inpatient setting, particularly in the context of acute medical conditions. This case highlights a novel hospitalist-led strategy and adds to existing evidence that the overlapping method of using full opioid agonists with low doses of buprenorphine can be effective in achieving pain control. The pharmacodynamics and pharmacokinetics of extended-release morphine provide prolonged opioid coverage and minimize the rapid peaks and troughs of short acting opioids, reducing breakthrough withdrawal and cravings, potentially making it a more favorable option for patients with OUD. For hospitalists managing medically complex patients—including those with chronic pain, fentanyl exposure, and concurrent acute illness—this approach provides a practical pathway to stabilize symptoms while facilitating transition to maintenance treatment with medications for OUD (MOUD). By default, most patients with uncontrolled pain are started on short-acting opioid agonists in the inpatient setting, which may perpetuate withdrawal and delay MOUD initiation. Implementing a protocol such as this allows hospitalists to balance effective pain control for management of patients’ acute issues with long-term recovery goals. Given that 1 in 9 hospitalizations involve a substance use disorder, expanding hospital-based addiction care is critical to improving medication adherence, reducing hospital readmissions, and promoting sustained engagement in treatment after discharge.
Conclusions: Hospitalists can improve outcomes for patients with OUD by integrating addiction treatment with acute medical care. Implementing an inpatient protocol with extended-release morphine bridging to low-dose buprenorphine initiation can enhance pain control, reduce withdrawal and cravings, and facilitate sustained engagement in long-term treatment.