Case Presentation: A 27-year-old woman with history of hypertension, diabetes mellitus, hyperlipidemia, and family history of sudden cardiac death presents to the hospital with complaints of substernal chest pain and palpitations. She has a history of recurrent chest pain following multiple COVID-19 infections. Labs were unremarkable except uncontrolled glucose level. Electrocardiogram demonstrated normal sinus rhythm. Echocardiogram demonstrated normal ejection fraction of 66%.She underwent coronary imaging which demonstrated a long intramuscular segment of the left anterior descending artery. She then underwent a coronary angiogram which revealed hemodynamically significant myocardial bridging of the left anterior descending (resting-full-cycle-ratio, RFR 0.76), moderate lesions involving the 1st diagonal and 1st/2nd obtuse marginals. She was placed on medical therapy with beta-blockers and calcium channel blockers without significant improvement.Cardiothoracic surgery did not feel that an unroofing procedure would be adequate given the length of the intramuscular segment and therefore opted to do a 3-vessel coronary artery bypass with left internal mammary artery to the diagonal and left anterior descending and right internal mammary artery to the obtuse marginal branch. She had an uneventful post-operative course and had full relief of symptoms.
Discussion: Myocardial bridging occurs when a portion of the epicardial coronary artery tunnels underneath a band of myocardium. Myocardial bridging can be asymptomatic or cause a variety of complications including acute coronary syndrome, coronary vasospasm, ventricular septal rupture, and arrhythmias. The most commonly involved epicardial coronary artery is the left anterior descending usually the middle segment. Myocardial bridging has largely been considered a benign condition however symptomatic patients who are refractory to medical management often undergo surgical intervention with unroofing procedures and rarely coronary artery bypass graft surgery.
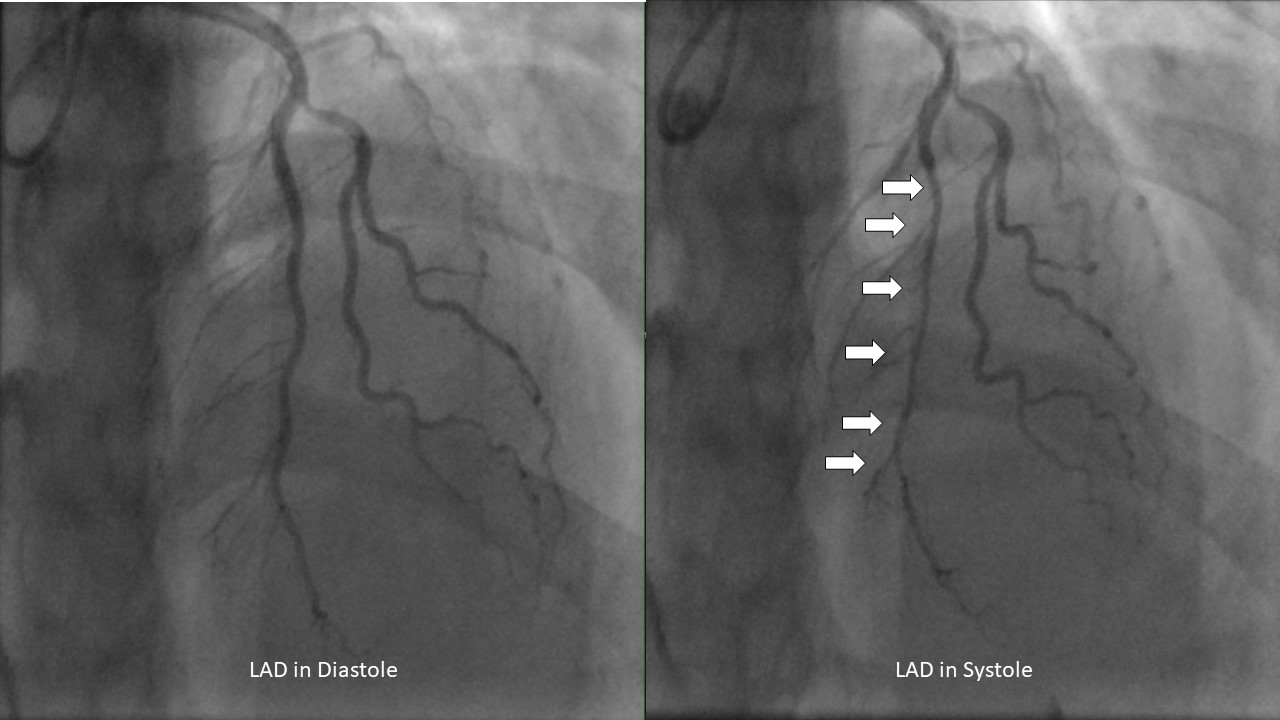
Conclusions: Myocardial bridging is diagnosed by coronary angiography with systolic narrowing of the epicardial coronary artery. The prevalence of myocardial bridging occurs in approximately 1.3% of the general population. Symptomatic cases of myocardial bridging are often treated successfully with beta-blockers. However, in refractory cases it has been proposed that percutaneous stent placement can prevent external compression however in limited studies the rate of restenosis remains too high to be recommended in symptomatic patients. Surgical intervention with unroofing or coronary artery bypass grafting surgery remains relatively safe and the treatment of choice for myocardial bridging.