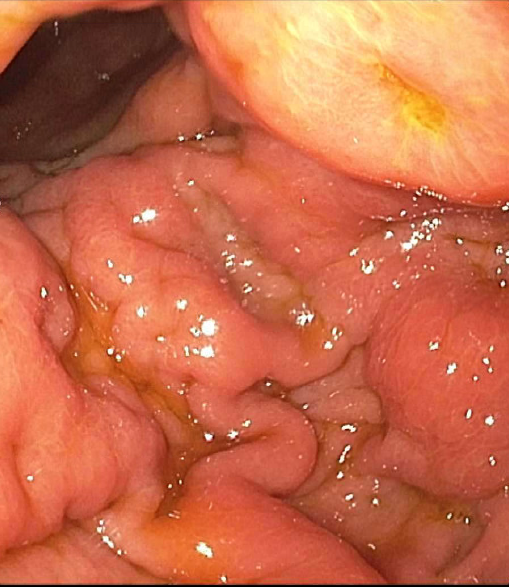
Case Presentation: A 73-year-old woman with a history of cervical carcinoma treated with chemotherapy and radiation in remission presented with weight loss (6 kg), poor oral intake and dysphagia over the prior three months. She reported epigastric and chest discomfort after swallowing, early satiety and the feeling of food becoming stuck in her upper abdomen. These symptoms occurred with both solids and liquids. She also reported fatigue, weakness, and night sweats.On examination the patient had temporal muscle wasting, dry mucus membranes and hypotension. Abdomen was mildly distended but soft with mild epigastric tenderness. The rest of the examination was unremarkable. Computed tomography (CT) of the abdomen and pelvis revealed bilateral hydronephrosis, uterine and bladder masses and a peritoneal implant close to stomach with drop-down metastasis on Douglas cul-de-sac. Findings on esophagogastroduodenoscopy included diffuse and patchy moderate inflammation characterized by congestion (edema), erosions, erythema, friability, granularity and shallow ulcerations suspicious for linitis plastica (Figure). Tissue biopsy was performed of the stomach mucosa and of the bladder mass revealing poorly differentiated p16-positive squamous cell carcinoma likely of anogenital origin. It remained unclear due to the poorly differentiated nature of the tumor if this represented a recurrence of cervical cancer or a new genitourinary primary site. She was begun on palliative chemotherapy with paclitaxel and carboplatin.
Discussion: Linitis plastica (LP), or “leather bottle” stomach, a term used to describe the gross appearance of the stomach, referring to the lmited distensibility of the stomach walls, is a rare complication traditionally associated with gastric cancer. The condition arises from diffuse infiltration of tumor through the layers of the gastric wall leading to rigidity and thickening. The term “linitis” refers to microscopic appearance of bands of filaments resembling linen cloth. Notably the layers involved are the submucosa and muscularis propria, often sparing the superficial mucosal layer. Secondary linitis plastica, arising from metastasis from another tumor site as in this case, is extremely rare and has been reported with colon, ovarian and breast cancer. Presenting symptoms include dyspepsia, dysphagia, nausea, vomiting and anorexia usually arising in an insidious manner over time. Diagnosis is confirmed by endoscopy but may be missed due to lack of mucosal involvement and non-diagnostic biopsies. Endoscopic ultrasound may help identify areas of irregularity in the submucosal regions. CT and MRI also have a role in diagnosis and may reveal gastric wall thickening as well as other areas of tumor involvement. Unfortunately, LP confers a worse prognosis as the tumor tends to be more aggressive and is associated with higher stage disease on presentation. Our patient’s dysphagia began to improve with initiation of chemotherapy but nausea related to therapy remained an issue.
Conclusions: Linitis plastica is a rare malignant cause of dysphagia and weight loss, associated with gastric cancer in the primary form but may arise from metastatic disease in its secondary form. Hospitalist practitioners should be aware of the pitfalls in diagnosis of this rare disorder.