Background: The Saga Fall Risk Model 2 (SFRM-2) is a simple fall prediction model using eight easily evaluated items upon admission in acute care hospitals (Figure 1). In a prospective validation study conducted at two acute and chronic care hospitals, the overall area under the curve (AUC) of SFRM2 was 0.793. However, it varied between hospitals, with 0.822 in the acute care hospital and 0.642 in the chronic care hospital, indicating differences in the SFRM2 accuracy between hospitals. Patients in long-term care hospitals have poorer activities of daily living and a higher risk of falls than those in acute care hospitals. Although effective fall predictive models exist for long-term care hospitals, their accuracy remains suboptimal. This study aims to validate the SFRM-2 in long-term care hospital patients.
Methods: This multicenter retrospective observational study was conducted in three long-term care hospitals in Japan from April 2018 to March 2021. All inpatients aged ≥20 years were included. The eight items of the SFRM-2 (age, sex, emergency admission, department of admission, hypnotic medication use, history of falls, eating independence, and Bedriddenness rank) and in-hospital falls were collected from medical records. Bedriddenness rank is an official ADL indicator used in Japanese medical and nursing care settings. This study evaluated Bedriddenness rank in five major categories (normal, J: independence/autonomy, A: housebound, B: chair-bound, or C: bed-bound). Benzodiazepines and non-benzodiazepines were included among hypnotic medications, except for melatonin receptor agonists and orexin receptor antagonists. The accuracy of SFRM2 was assessed by calculating the area under the curve (AUC) and shrinkage coefficient, as well as the sensitivity, specificity, positive predictive value, and negative predictive value.
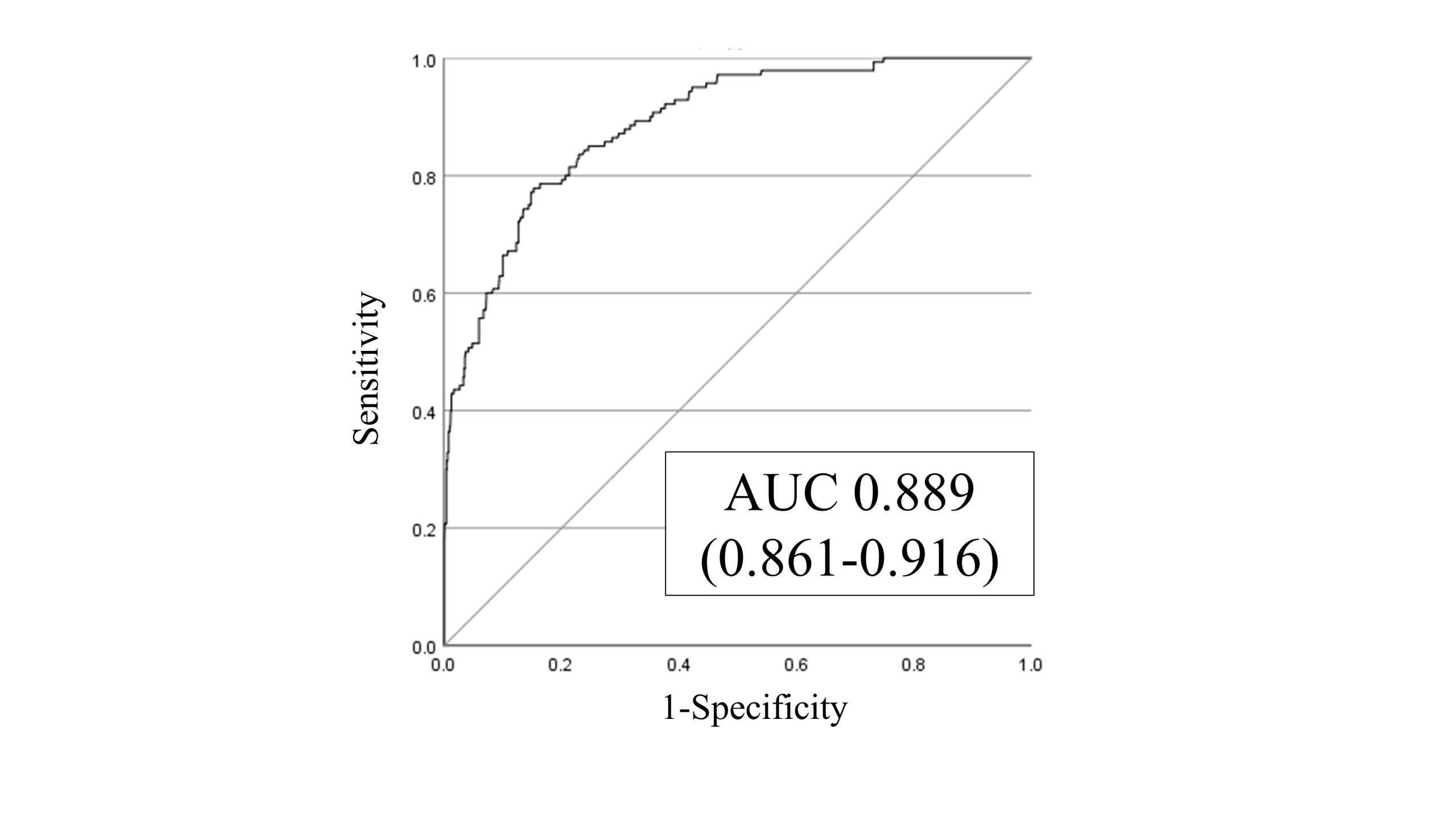
Results: A total of 1,182 patients were included in the analysis. The median age was 86 years, and 45.5% were male. The median length of hospital stay was 27 days. A total of 140 falls occurred (11.8%), with an incidence rate of 4.4 per 1,000 patient-days. Within the fall group, the median age was 88 years, 79.3% were male, and the median length of hospital stay was 68 days. SFRM-2 exhibited an AUC of 0.889 (95% confidence interval: 0.861-0.916) (Figure 2), consistent with the actual incidence of falls, with a shrinkage coefficient of 0.975. The cut-off score for SFRM-2 on the Youden index was -2.14, with a sensitivity of 77.9%, specificity of 84.7%, positive predictive value of 40.6%, and negative predictive value of 96.6%.
Conclusions: SFRM-2 demonstrated high discriminatory power in external validation for long-term care hospitals. Its applicability in this setting may be advantageous die to the relatively stable condition of older inpatients as compared to those in acute care hospitals.