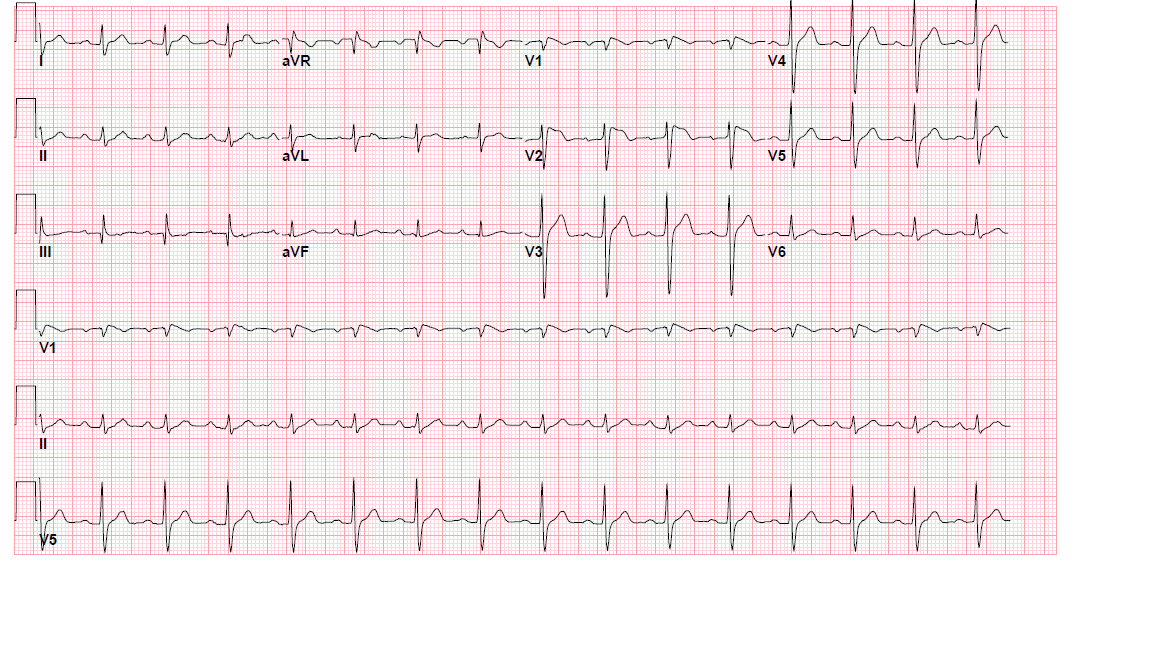
Case Presentation: A 57-year-old Hispanic man with a past medical history of essential hypertension and nephrolithiasis, presents to the emergency room with a witnessed syncopal event lasting less than a minute. He also refers a two day history of subjective fever and dysuria associated with nausea and anorexia. Further review of systems was unremarkable. He specifically denied any history of chest pain, dyspnea, dizziness, palpitations, or prior similar episodes. Family history did not include episodes of sudden death or cardiac arrest. On physical exam, the patient did not appear to be in acute distress. He was febrile (39.3°C) and tachycardic (heart rate 110 bpm). All other vital signs were within normal limits. The remainder of the physical examination was unremarkable. Laboratory values on admission were notable for a white cell count of 21.1 × 10−9/l and abnormal kidney function tests. Urine analysis revealed elevated leukocyte esterase and pyuria. Urine culture later grew pansensitive Escherichia Coli. Electrolytes, and troponin values were within normal limits. Chest x-ray was unremarkable. Blood cultures were negative. EKG revealed sinus rhythm at 96 bpm with a coved ST segment elevation in leads V2 and V3, consistent with a Brugada pattern. He was treated with IV ceftriaxone and placed on continuous cardiac monitoring. Echocardiogram was normal. Cardiology was consulted and an electrophysiology study was performed, which confirmed the diagnosis of Brugada syndrome. An implantable cardiac defibrillator (ICD) was placed before the patient’s discharge. EKG re-evaluation when patient was afebrile, showed no ST segment elevation.
Discussion: Brugada syndrome is an inherited arrhythmia caused by mutations in the sodium and calcium channel genes. These cellular abnormalities do not distort myocardial structure, resulting in normal cardiac examinations, including echo-cardiogram and cardiac MRI. It is a major cause of ventricular arrhythmias and sudden death in young people. The condition was first described in 1992, and since then, many reports have identified diverse provoking factors: medication and toxins, electrolyte imbalance and of course, fever. Fever was identified as the trigger in about 18% of the cardiac arrests in patients with symptomatic Brugada syndrome.
Conclusions: Early prevention of malignant arrhythmias is the key principle guiding the therapy of Brugada syndrome. However, due to its transient nature, EKG changes may still be under recognized. Our case represents a common scenario in the inpatient setting. Fever is an important trigger that may unmask EKG changes and raise suspicion for Brugada syndrome. Due to the potential fatal consequences, active vigilance should be maintained when fever and syncope present together.