Background:
Critical lab values are those results that require rapid notification to clinical staff so that urgent interventions can be made to avoid morbidity or mortality. The Joint Commission requires that hospitals have an effective critical lab value process in place. The process is a time-consuming multi-step progression of phone calls with associated documentation. The components of the critical lab value list are left up to each institution.
Patient safety incident reports led hospital leadership to raise concerns regarding our institution’s critical lab value process. A hospitalist led multi-disciplinary quality improvement team was commissioned to perform a comprehensive review of the critical lab value process. The team consisted of a hospitalist, a clinical pathologist, and nursing leadership.
Purpose:
To describe how a hospitalist led multi-disciplinary quality improvement team reviewed the existing critical lab value process and implemented effective improvements
Description:
Evaluation of the existing critical lab value process revealed a dysfunctional system with too many critical lab tests, poor documentation, and a lack of ongoing review of the process. Additionally, the overwhelming number of critical lab values was leading to alarm fatigue on the part of frontline clinical staff. The review validated hospital leaderships concerns regarding the effectiveness of the process.
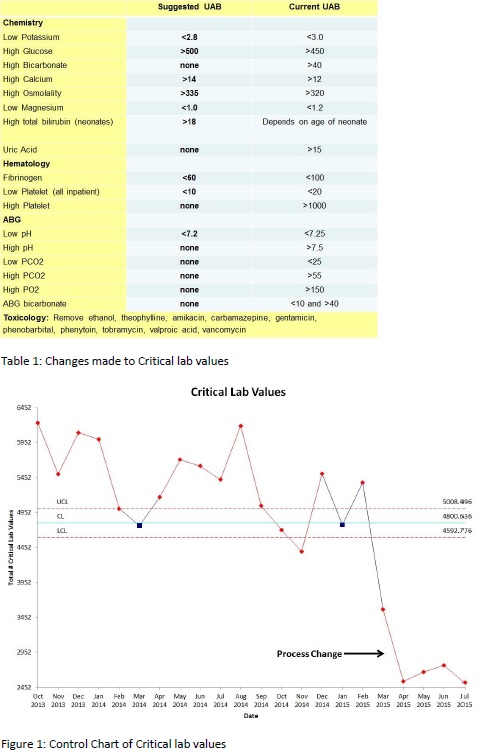
The team gathered ten specialist physicians with pertinent expertise and outstanding clinical reputations to serve as a local expert committee to revise the critical lab value list. During a single one hour session, each lab and parameter on the current list was reviewed by the committee. The committee made recommendations for modifying the list and consensus was reached via subsequent email discussion (Table 1). The recommendations of the committee were then presented to and accepted by hospital administration.
The control chart shows the process change that occurred after implementation of the revised list (Figure 1). The process change has led to an approximately 50% decrease in number of critical lab values. An estimated 1.8 full-time equivalents of laboratory technician has been saved and is hence available for more useful activities that will benefit patient care. Additionally, frontline clinical and laboratory staff has been very enthusiastic about the improvement, likely due to a reduction in alarm fatigue. Patient safety monitoring is ongoing and no related adverse events have been reported.
Conclusions:
An overburdened critical lab value process can decrease its utility and lead to alarm fatigue. A hospitalist led multi-disciplinary quality improvement team can facilitate improvements in this process. Facilitating a committee of local experts to review and revise the components of the critical lab value list was an effective means of improving this process.