
Background: Clinical documentation is a major contributor to hospitalist burnout due to the time spent on note writing and chart review. Generative artificial intelligence (AI) may help reduce this burden, yet most tools offer limited control over source information or output structure. Additionally, little is known about how clinicians actually use these tools in practice or which clinical tasks benefit most.
Purpose: To evaluate an electronic health record (EHR)-native generative AI tool with two goals: 1) assess its perceived impact on documentation burden and efficiency, and 2) characterize real-world use to identify documentation tasks where AI support is most helpful.
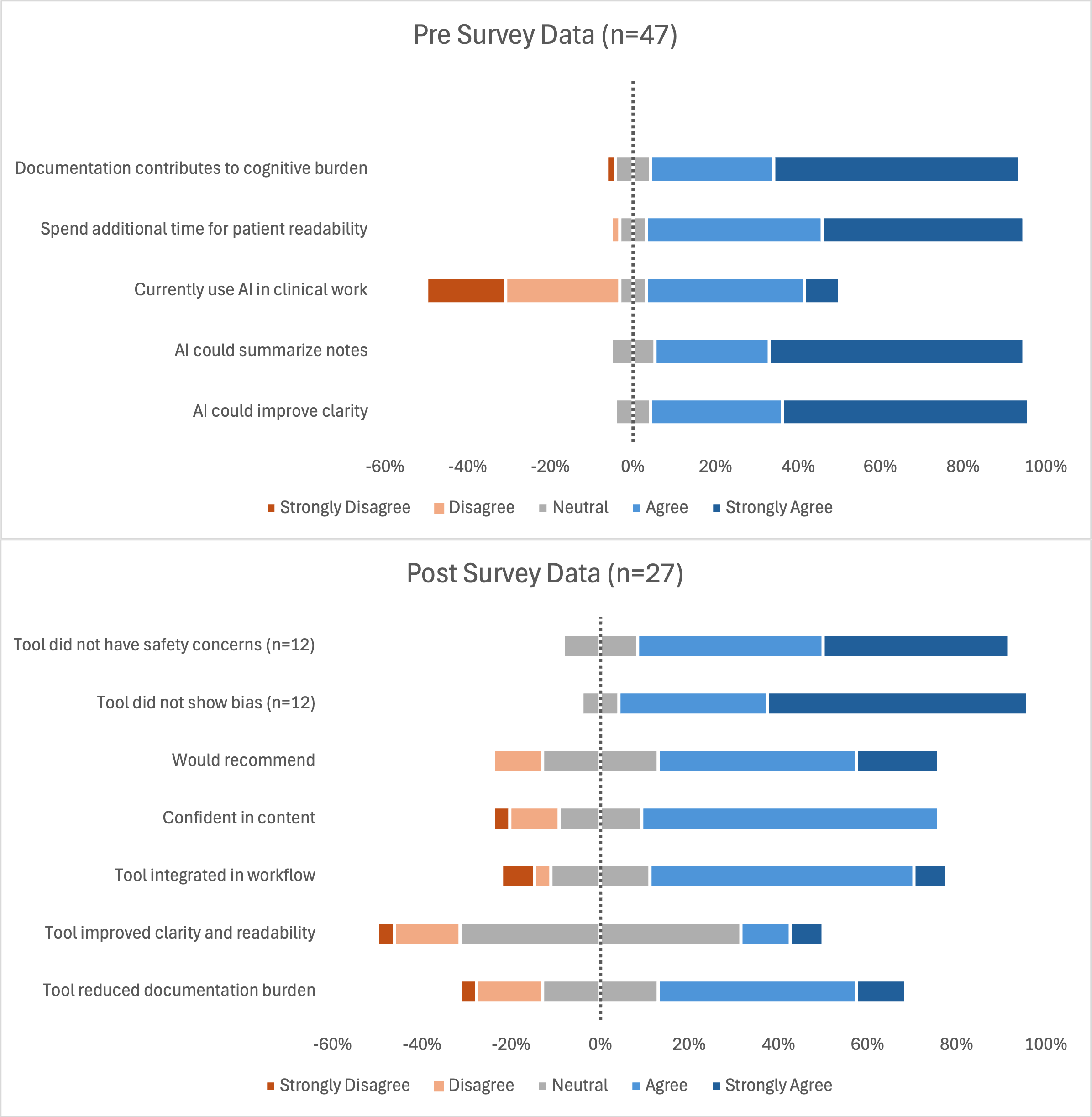
Description: A multidisciplinary team of clinical informaticians, hospitalists, and AI specialists launched an AI Text Assistant that summarized, rephrased, and formatted clinical text, while allowing users to select source information within the note. Implementation included a structured validation phase followed by a three-month inpatient pilot. During validation, two hospitalists independently reviewed outputs with high agreement for accuracy (86%) and usability (88%). In the pilot (1,028 uses, 47 hospitalists), providers accepted the output 75% of the time, modified it 18%, and rejected it 7%, suggesting the tool produced clinically usable text with minimal editing. The most frequent request was “Summarize: use clinical language,” accounting for 70% of all uses with 81% acceptance. Usage patterns reflected heavy reliance on the assistant for cognitively demanding tasks; clinicians mainly used summarization to create hospital courses, attestations, and discharge summaries.47 providers completed a pre-use survey to assess baseline attitudes toward time spent on documentation and the use of AI, and 27 (57%) completed a post-use survey after using the initial version of the tool. Preliminary results demonstrated an overall positive impact: 56% reported reduced documentation burden, 67% reported effective workflow integration, and 63% would recommend the tool. Qualitative feedback indicated a desire for improved control over writing style, tone, and formatting. In response to the survey findings, the implementation team expedited the deployment of the newest version of the tool which added a custom prompt feature. This update was not originally planned for the pilot but was directly aligned with requests for further customization of the output. Early use of the updated version shows even broader applications than before, including the creation of provider handoffs and individualized discharge instructions. In one creative example, a provider embedded billing guidelines into a custom prompt that extracted and labeled medical decision-making elements directly from a progress note.
Conclusions: An EHR-native AI documentation tool that allows users to control source information demonstrated high accuracy, strong acceptance, and perceived reductions in documentation burden. Real-world use showed that hospitalists primarily rely on AI for complex documentation tasks. The decision to deploy custom prompts in response to user feedback underscores the importance of adaptable, clinician-driven implementation strategies that can enhance trust, usability, and long-term adoption in inpatient settings.
.png)