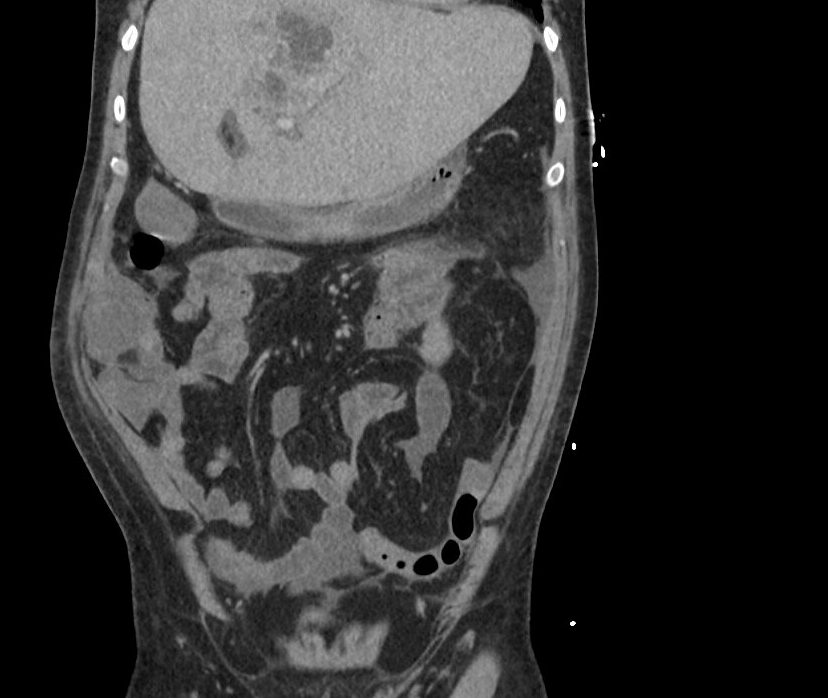
Case Presentation: A 60-year-old male with a history of right hepatic resection for donation in 2011 presented to theEmergency Department for acute onset of chills, malaise, and fever up to 101.3 at home withassociated vomiting, abdominal pain, and abdominal distention. He was found to have fluidrefractory hypotension, elevated lactate, and a stage II AKI with CT concerning multiplehepatic abscesses. He was started on vasopressors, and broad-spectrum antibiotics, and admitted tothe medical ICU for septic shock. His shock resolved in less than 24 hours and he was transferredto the medical floor.His abscesses resulted in intrahepatic biliary obstruction, later managed with percutaneous drainagegiven the high-risk location. Cultures of the aspirate and blood grew F. nucleatum. Follow-up CTwas remarkable for a hyperattenuating mucosal lesion in the cecum. A colonoscopy wasperformed, and remarkable for a Paris 0-IIa+c lesion (flat elevation with central depression).Pathology was consistent with invasive adenocarcinoma. The biopsy was complicated byrecurrent hemorrhage. He underwent a right hemicolectomy with end ileostomy for definitivemanagement of both his malignancy and GI bleeding. Final surgical pathology showed adenocarcinomainvading the muscularis propria with negative margins. Throughout his stay, he was managedwith Piperacillin/Tazobactam followed by Metronidazole and Ciprofloxacin upon discharge withserial imaging to guide the duration of therapy.
Discussion: Colorectal cancer accounts for 150,000 cases of newly diagnosed cancer in the United States andleads to over 50,000 deaths annually. The 5-years survival rate of colorectal cancer hassignificantly improved following the widespread adoption of preventative cancer screening.Recent research has shed light on the association of gut microbiota with carcinogenesis inCRC. As an example, Streptococcus gallolyticus, previously S. bovis, and its association withCRC has been known since 1951. F. nucleatum is an anaerobic commensal gram-negative bacterium that colonizes both thegastrointestinal and respiratory tract. The increased colonization in patients with CRC compared to healthy individuals has raisedconcerns about its role in oncogenesis. Proposed mechanisms include the production of virulencefactors Fap2, which promotes bacterial proliferation and affinity for CRC, and FadA, whichupregulates the oncogenic ß-catenin signaling pathway. F. nucleatum has been proposed topromote CD11b+ myeloid cell proliferation and NK cell inactivation, aiding angiogenesis andevasion of immune destruction respectively.
Conclusions: In this case report, we discuss a case of multiple pyogenic liver abscesses and bacteremia secondary to Fusobacterium nucleatum (F. nucleatum) prompting a subsequent diagnosis of colorectal cancer. This case highlights the uncommon initial presentation of bacteremia and hepatic abscess formation in patients with CRC. Identification of F. Nucleatum infection in a patient should be followed by prompt evaluation for colonic malignancy. stool DNA testing of F. Nucleatum was pioneered in Japan as a possible screening tool for patients at risk of developing CRC. Research into intestinal dysbiosis and its role in oncogenesis is a rapidly expanding field. Further research may help guide the identification of additional culprit organisms and aid in risk stratification.