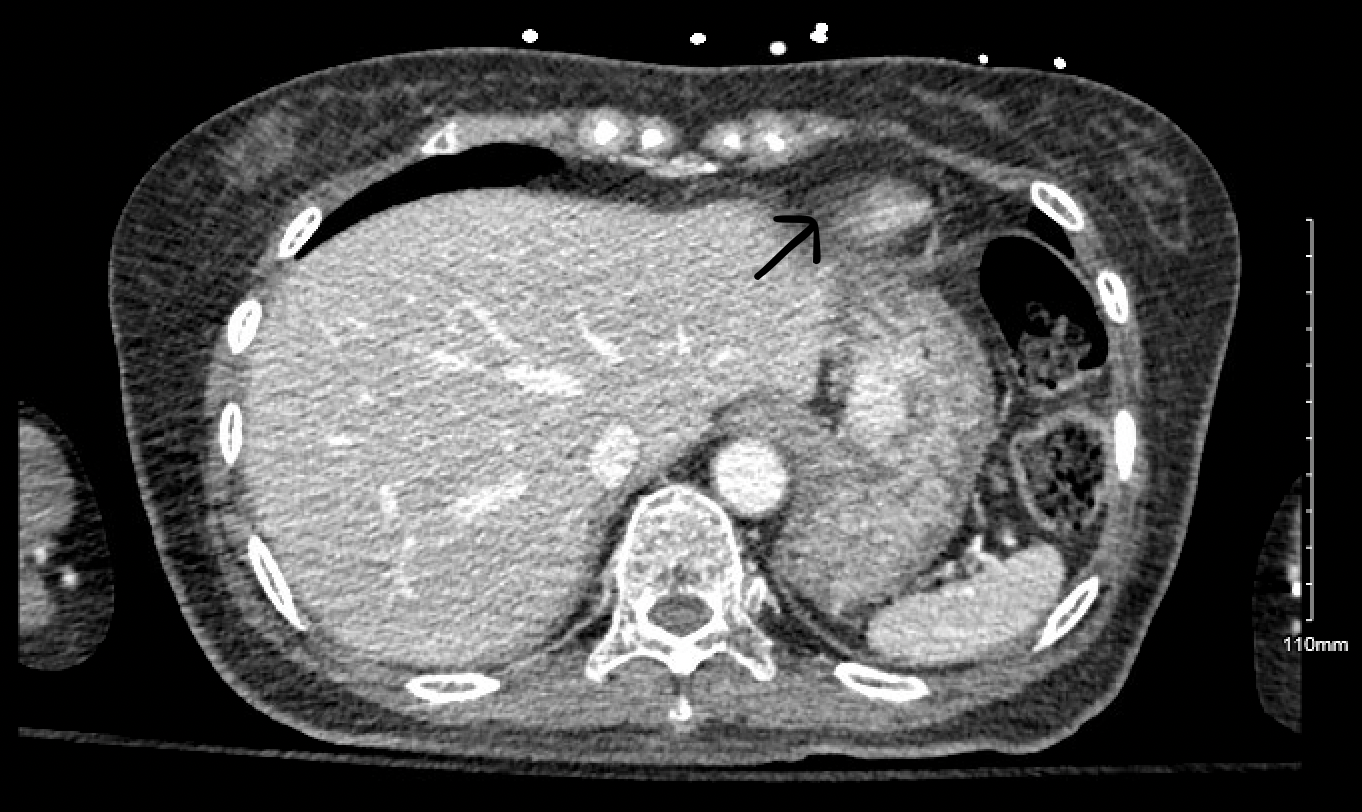
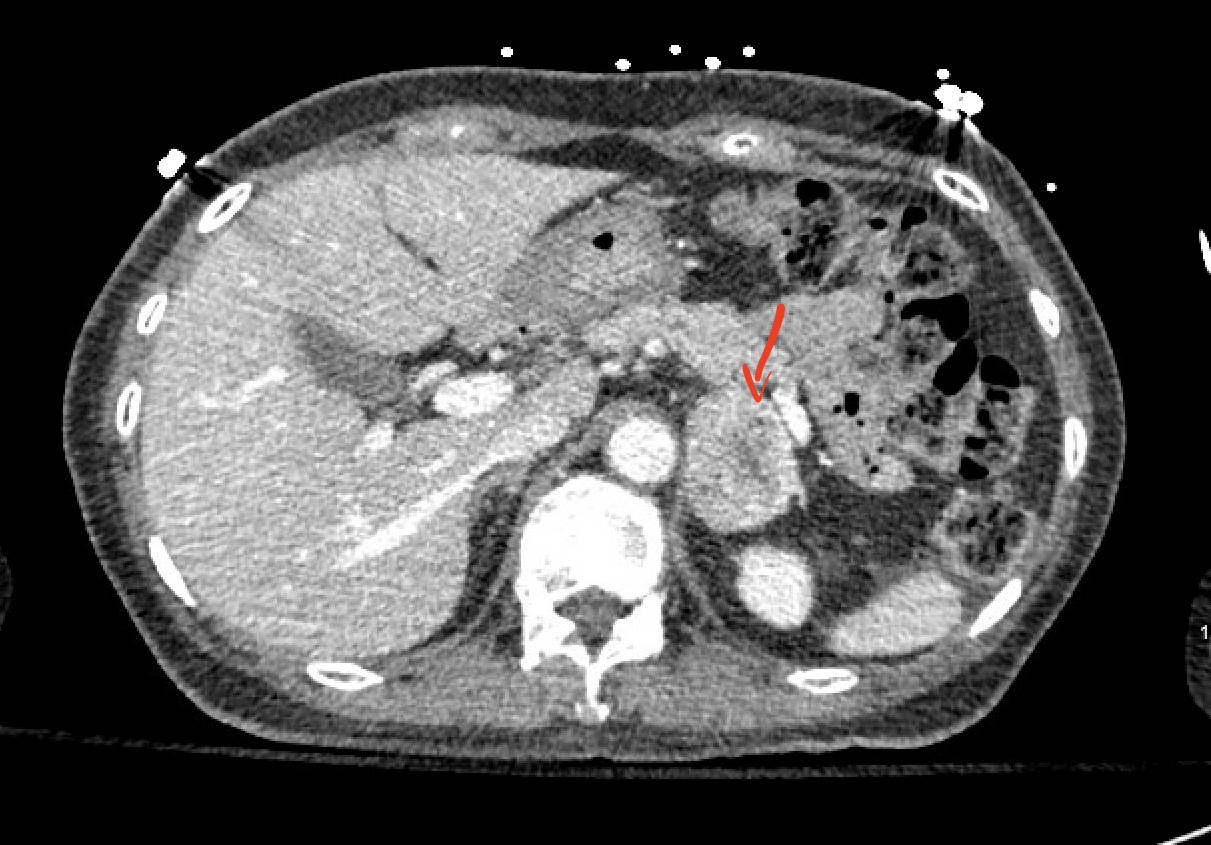
Case Presentation: This is a 72-year-old female patient who presents to the ED for the evaluation of loss of consciousness. The patient’s family also endorsed dark stools for the past few days. She has a medical history significant for Insulin Dependent Diabetes Mellitus, and papillary thyroid cancer. On arrival, the Patient’s BP was 126/55, Heart rate of 74bpm, Afebrile, and saturating 96% on room air. Physical examination was unremarkable. Laboratory studies show hemoglobin of 6.4 g/dl, Platelet count of 132,000, INR of 1.0, blood glucose of 274 mg/dl, BUN; 51mg/dl, and Creatinine 0.65. Testing for occult blood came out to be positive. CT Head was done which was negative for any acute intracranial hemorrhage. The patient underwent an Upper GI Endoscopy which was consistent with subepithelial gastric lesions on the lesser curvature and body of the stomach with extensive lymphadenopathy suspicious of Gastrointestinal malignancy. Fine needle Aspiration biopsy was done during the procedure which showed spindle cell neoplasm supporting the diagnosis of GIST. CT Chest Abdomen & Pelvis was done to evaluate for any metastasis which showed a left-sided adrenal mass (Image 1&2). The adrenal mass was biopsied subsequently which came out to be positive for a neuroendocrine tumor. Urine and serum metanephrines & normetanephrine levels, ordered before the surgical intervention, were found to be elevated. The patient was initially treated with phenoxybenzamine and eventually underwent gastrectomy.
Discussion: Gastrointestinal stromal tumors (GISTs) represent less than 1% of all gastrointestinal tract tumors. GISTs have been described to coexist with other neoplasms, with the percentage of such cases ranging from 4.5% to 33%. The most frequent concomitant tumor is adenocarcinoma of the gastrointestinal tract; other types include lymphoma, leukemia, carcinomas of the breast, prostate, pancreas, lung, or pheochromocytoma. Patients with a simple GI bleed and remote cancer history when found to have a neuroendocrine tumor in the GI tract should always be screened for other associated malignancies.
Conclusions: GIST with associated pheochromocytoma is typically found in patients with neurofibromatosis type 1. Here in our case, the patient was found to have a GIST with synchronous pheochromocytoma without neurofibromatosis. This is a simple reminder to all clinicians about the importance of screening for associated cancers in all patients diagnosed with GIST.