Background: Due to medical complexity, children with complex chronic conditions (CCC) have high hospital mortality rates. End-of-life (EOL) care planning is critical for these children and requires collaboration with families. Despite the importance of EOL care aligned with patient/family goals and potential harm when EOL care is inconsistent with these goals, there is limited literature on the delivery of goal-concordant EOL care for children.
Methods: The objectives of this study were: (1) to characterize delivery of goal-concordant EOL care among hospitalized children; and (2) to determine the association between receipt of goal-concordant EOL care and level of medical complexity.We conducted a retrospective cohort study of 272 children who died at a tertiary care hospital between January 2014 and December 2017. Inclusion criteria were: age <19 years old, death while admitted, and ≥1 CCC. We defined CCCs with Feudtner, et al.'s classification system as a condition expected to last ≥12 months and involving either multiple organ systems or 1 system severely enough to require specialty pediatric care and likely hospitalization in a tertiary care center.We conducted a structured manual review of electronic health record notes to characterize goals of care (GOC) discussions conducted >72 hours before death and within the last 72 hours of life. We categorized each GOC discussion as follows: (1) full interventions without withdrawal of life support; (2) consideration of withdrawal of interventions but no immediate decisions; (3) planned transition to comfort care or withdrawal of life support; or (4) actively transitioning/transitioned to comfort care or withdrawing life support. We collected data on code status before and within the last 72 hours of life.
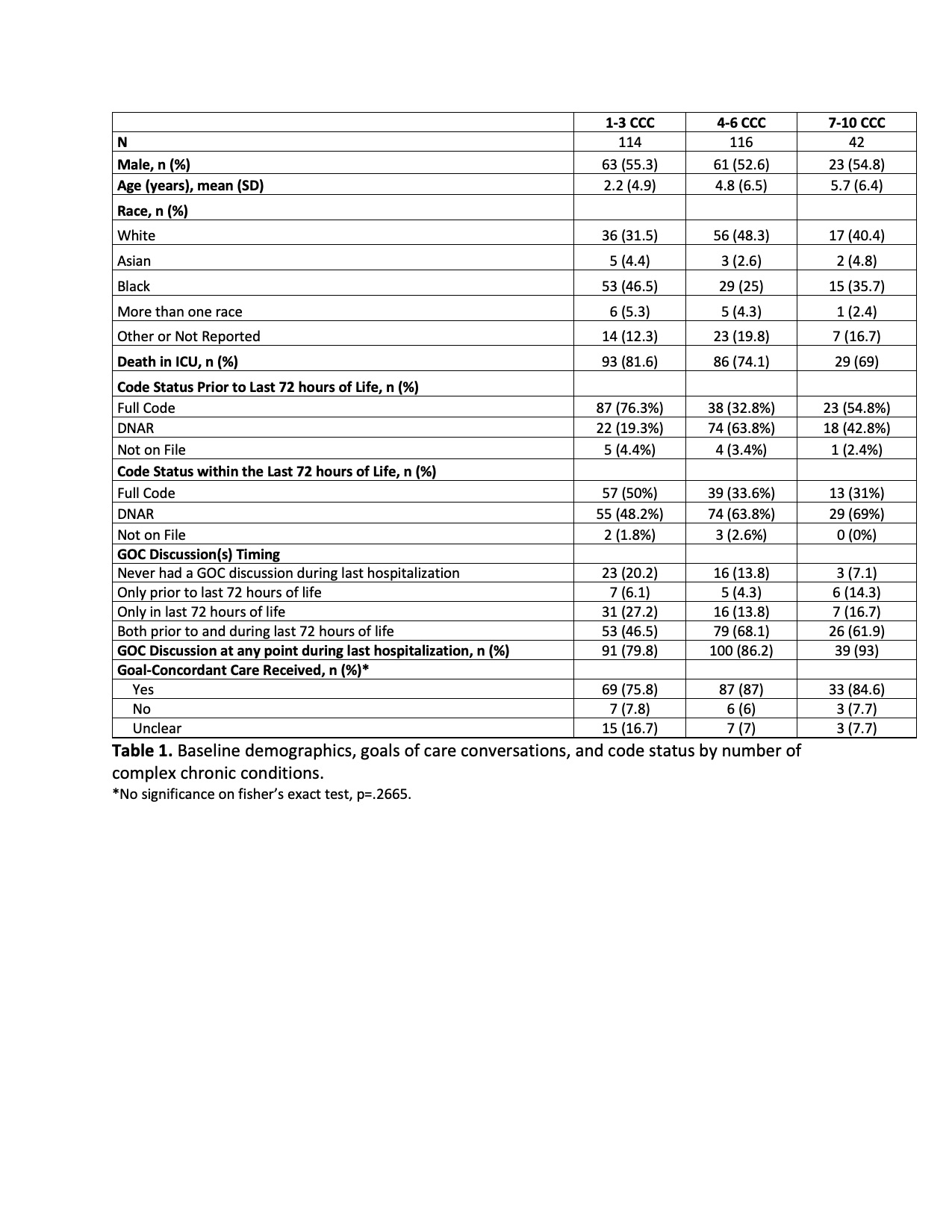
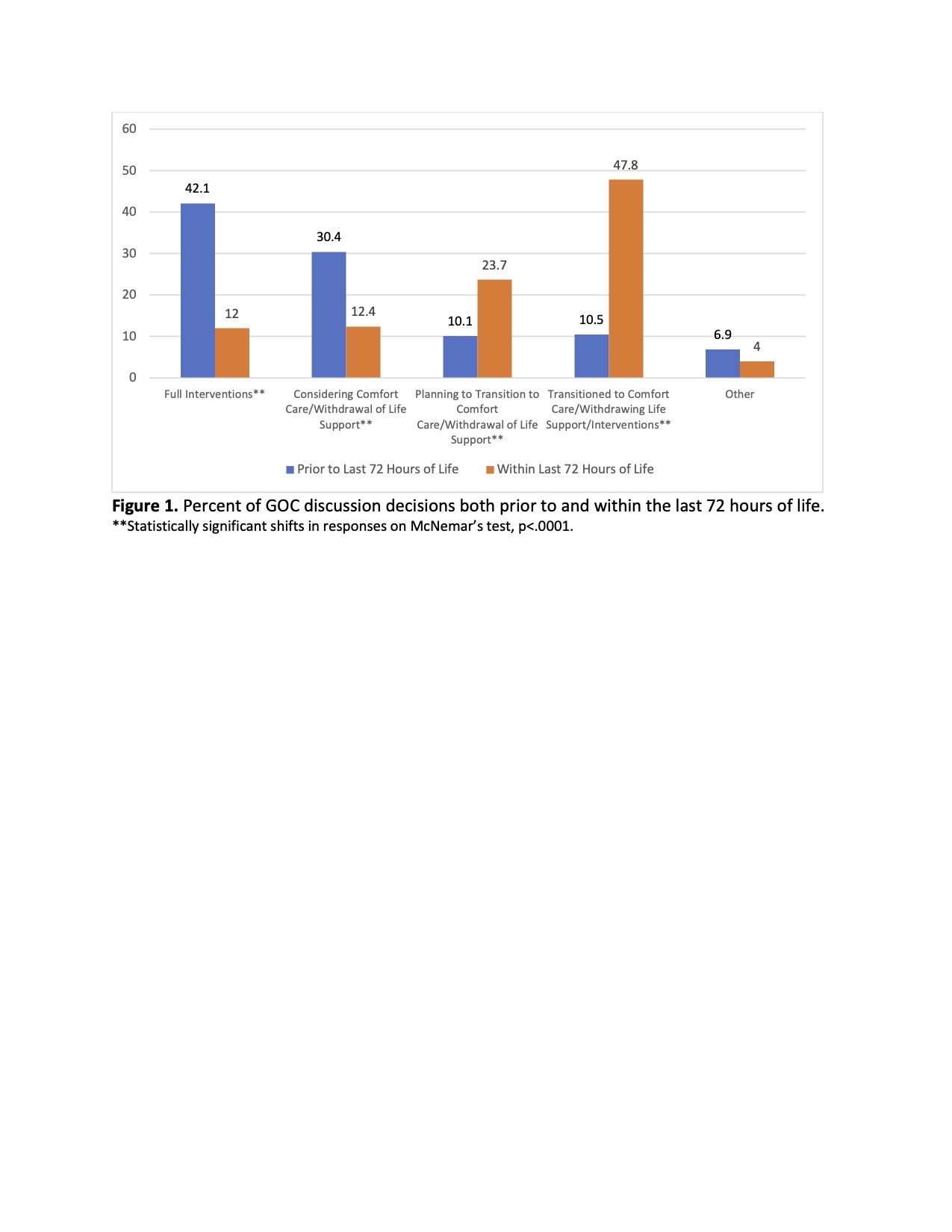
Results: Children in this cohort had an average of 4.1 CCCs (standard deviation, SD, 2.1), mean age of 3.9 years old (SD 6) and 76.5% died in the ICU (Table 1). 18 patients (6.6%) had GOC discussions only >72 hours before death, 54 (19.9%) had GOC dicussions only in the last 72 hours of life, 158 (58.1%) had documented GOC discussions both before and within the last 72 hours of life, and 42 (15.4%) had no documented GOC discussions during the last admission of life. Based on GOC discussions, EOL care was goal-concordant in 189 (82%), discordant in 16 (7%) and unclear in 25 patients (11%). Goal concordant EOL care was not associated with the number of CCCs (p=0.2665).Between the two time points: >72 hours before death and in the last 72 hours of life, statistically significant changes were found for the proportion of GOC discussions focused on planning (10.1% vs 23.7%) or actively transitioning/transitioned to comfort care/withdrawal of life support (10.5 vs 47.8%) on McNemar’s test (p values <.001). Likewise, significant reductions in the proportion of discussions focused on full interventions (42.1% vs 12%) or considering options (30.4% vs 12.4%) were found (p values <.0001) (Figure 1). Approximately 68% of the cohort had the same code status at both time points while 28% shifted from full code status >72 hours before death to do not attempt to resuscitate (DNAR) in the last 72 hours of life. These shifts were significant based on Bower’s test of symmetry (p<.0001) (Table 1).
Conclusions: In our study, 85% of children had documented GOC prior to death, but 1 in 7 children did not. Of those with GOC documented, 82% received goal-concordant EOL care and goal-concordance was not associated with higher medical complexity. GOC and code status shifted toward palliation in the last 72 hours of life.