Background: End-of-service handoffs on inpatient general medicine services occur when there is a transfer of care to new providers, often at the end of a scheduled rotation. This is high-risk time for patients as increased in-hospital mortality has been observed around the time of end-of-service handoffs. The Society of Hospital Medicine recommends use of a template or technology solution in addition to an interactive verbal exchange during all patient handoffs, which extends to include end-of-service handoffs. At our institution, handoff at shift change follows these best practices, but little is known about how providers perform end-of-service handoffs as no standardized method has been enforced.
Methods: At a single urban, tertiary referral academic medical center, an anonymous multiple-response survey with free text was sent via e-mail to all internal medicine residents and interns (n = 104) and attending physicians on faculty (n = 64) who were scheduled on inpatient general medicine teaching services in the Fall 2019 quarter. Responses were collected during a 2-week window in September 2019. Survey items assessed the means of communication through which handoffs at inpatient service changes occur and an estimate of time spent during typical end-of-service handoff. A free text field captured what respondents would want included in an ideal standardized end-of-service handoff, and these narrative comments were analyzed qualitatively.
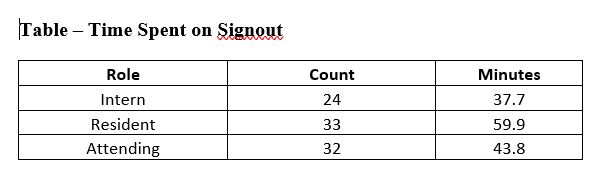
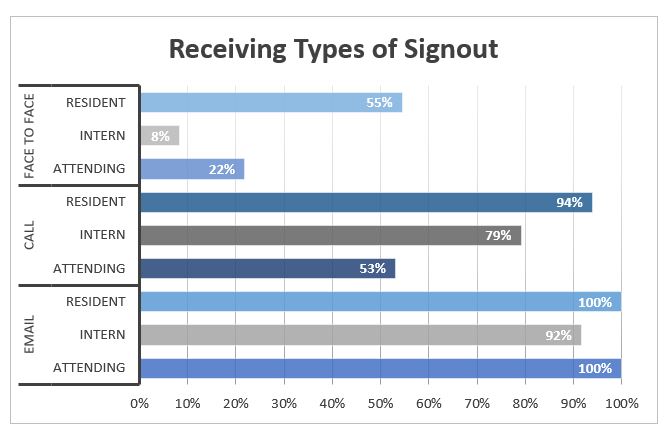
Results: Over 50% of residents and interns responded to the survey (56 out of 104) and 50% of invited attending faculty members (32 out of 64). Few respondents (2% of overall respondents) reported using a standardized template at end-of-service handoffs. The majority of respondents reported that their end-of-service handoff had used email (95% of respondents). Residents reported spending a statistically significant greater amount of time on end-of-service handoffs (mean = 60 min.) compared to interns (mean = 38 min., p = 0.004) and attending faculty (mean = 43 min., p = 0.04). The most important concept noted in free-text responses as a part of an ideal end-of-service handoff was a “To-Do” list (59% of overall respondents) and a summary of the hospital course (54% of overall respondents). Many attending faculty (38% of attending faculty respondents) also requested information about unique family relationships and social issues which is not often a part of standardized end-of-service handoffs.
Conclusions: There is lack of a standardized template or means of communication for the handoffs at the time of service changes of general medicine teaching services at our institution. The residents, in their role as team leaders, spend the most time on end-of-service handoff compared to interns and attending faculty. More interactive verbal exchanges and a written template should be considered to minimize the risk of adverse events related to ineffective end-of-service patient handoff.