Background: Despite advances in pharmacologic care for side effects of Hematopoietic stem cell transplant, patients often suffer from long hospitalizations, multiple side effects including fatigue, insomnia, nausea, anxiety, and poor sleep. Non-pharmacologic treatments for side effects of therapy are attractive adjuncts due to a low side effect profile.
Purpose: To develop, implement and evaluate a pilot program of massage therapy on patients with hematologic malignancies admitted to the Bone Marrow Transplant (BMT) inpatient service at a large academic medical center.
Description: Patients were informed of the availability of massage therapy by either a provider (nurse, physician, social worker) or posters which were placed in patient bulletins on the hospital floor. An order set was created in the electronic health record to make the service fully automated. An experienced (>10 years) therapist provided a 20-30 minute sessions of Swedish massage each Tuesday to patients who had a consult request. No other staff was required. Sessions were conducted in patient’s rooms at the bedside. Source of funding came from 10,000 dollars raised by a small-donation crowdfunding campaign conducted the prior year.
Over an 11.5-month period, 128 massage consults were ordered and 134 massage treatments were given. 142 surveys were collected, with 106 unique patients and 3 anonymous surveys identified. In total, 59 men and 75 women had a massage. Some patients received multiple massages. Their average age was 58.6 years and length of stay 21.6 days (Table 1).
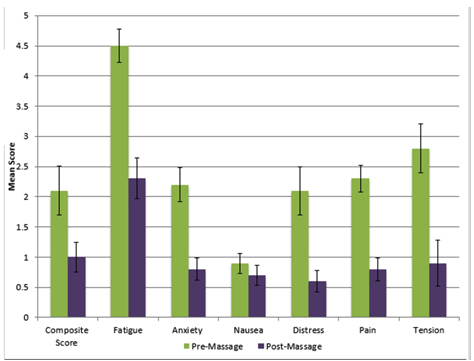
We evaluated the impact of the program by collecting pre and post massage surveys that assessed seven symptoms: pain, distress, tension, fatigue, sleep quality, anxiety, and nausea. These were assessed with a Wong-Baker 10-point rating scale. Sleep was assessed on a 4-point qualitative scale “worse, same, better, much better.” A free text comment section in the survey allowed patients to provide feedback on the experiences of massage during their hospitalization.
In an analysis of the composite outcomes of-anxiety-nausea-distress scores (Figure 1), patients reported statistically significant improvement post-massage (-1.16 95% CI: -1.55, -0.76; p<0.001). This improvement seems primarily driven by a reduction in reported fatigue, anxiety, and distress. Separately, patients reported significant reductions in pain and tension. 72% of patients also reported either “better” or “much better” sleep. No adverse effects were reported.
Free text survey comments were highly supportive of the massage program. Patients felt massage helped them relax, reduced their anxiety, improved their mood, and helped them manage their illness.
Conclusions: Based on this pilot, massage therapy is a feasible intervention to administer during BMT hospitalizations. It proved both useful and a safe adjunct to managing the constellation of side effects frequently encountered in this patient cohort. As a result of this pilot, massage therapy was permanently incorporated as a therapeutic modality in the adult BMT service.
.png)