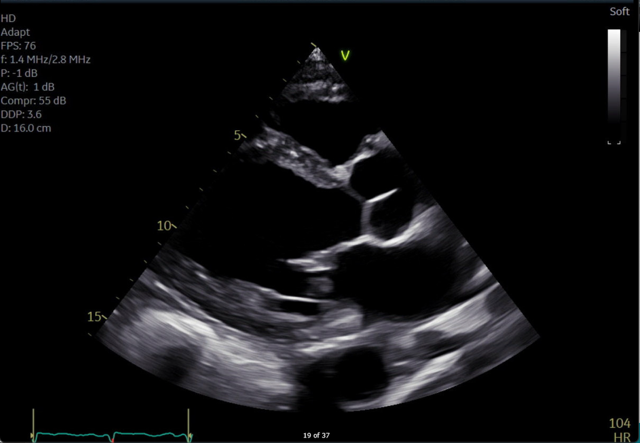
Case Presentation: A 63-year-old male with a history of heart failure with reduced ejection fraction (HFrEF), type 2 diabetes, and recent left below-knee amputation presented with worsening dyspnea, orthopnea, and leg swelling. Physical examination revealed volume overload with jugular venous distention and pitting edema. NT-proBNP was markedly elevated (10,901 pg/mL). Transthoracic echocardiography (TTE) showed a moderately dilated left ventricle with reduced systolic function (EF 36%), global hypokinesis, and reduced global longitudinal strain (-11.0%). Additional findings included severe left atrial dilation (volume index >48 mL/m²), mildly dilated right atrium, preserved right ventricular function despite dilation, and mild valvular regurgitation. Multisystem involvement and unexplained cardiomyopathy raised suspicion for Fabry disease. Genetic testing for GLA mutations was recommended, and the patient was managed with optimal heart failure therapy, including diuretics, ACE inhibitors, beta-blockers, and spironolactone. His diabetes management was also optimized.
Discussion: Fabry disease is a rare cause of nonischemic cardiomyopathy, often underdiagnosed in patients with diabetes or hypertension. These patients may have cardiac manifestations, including LVH, myocardial fibrosis, and reduced longitudinal strain, which can be challenging to recognize as it mimics other diseases. Ultimately, early diagnosis with genetic testing and enzyme activity assays is crucial for ERT initiation to prevent progression and improve outcomes. Abnormal features on echocardiography such as global hypokinesis, atrial dilation, and abnormal cardiac strain pattern should lead to consideration of Fabry disease in the setting of unexplained HFrEF. This case illustrates the importance of maintaining a high index of suspicion for systemic symptoms and a detailed echocardiographic examination.
Conclusions: Fabry disease should be considered in patients with unexplained heart failure, particularly with multisystem manifestations. Attention to echocardiographic imaging findings, when paired with systemic signs, can guide clinicians toward early diagnosis and targeted interventions like enzyme replacement therapy, potentially preventing irreversible organ damage. This case highlights the importance of maintaining a broad differential and paying close attention to diagnostic details to ensure timely and effective treatment for uncommon causes of HFrEF.