Case Presentation: A 24 year old pregnant woman presented at 32w1d with three days of fevers, chills and fatigue. Her pregnancy had been complicated by asthma, obesity, pyelonephritis, and a recent gonorrhea infection. Her vital signs on presentation revealed a temperature of 39.5°C, heart rate of 150, blood pressure of 101/67, respiratory rate of 44, and SaO2 of 96% on room air. Her physical exam was otherwise unrevealing. Initial labs were notable for new thrombocytopenia, anemia, and transaminitis (AST:383, ALT:200). She was admitted and treated for sepsis due to presumed chorioamnionitis. Her thrombocytopenia and transaminitis progressively worsened, and she was transferred to the intensive care unit for hemodynamic and respiratory support. With a leading diagnosis of atypical HELLP (hemolysis, elevated liver enzymes, low platelets), the patient had a C-section at 32w4d.
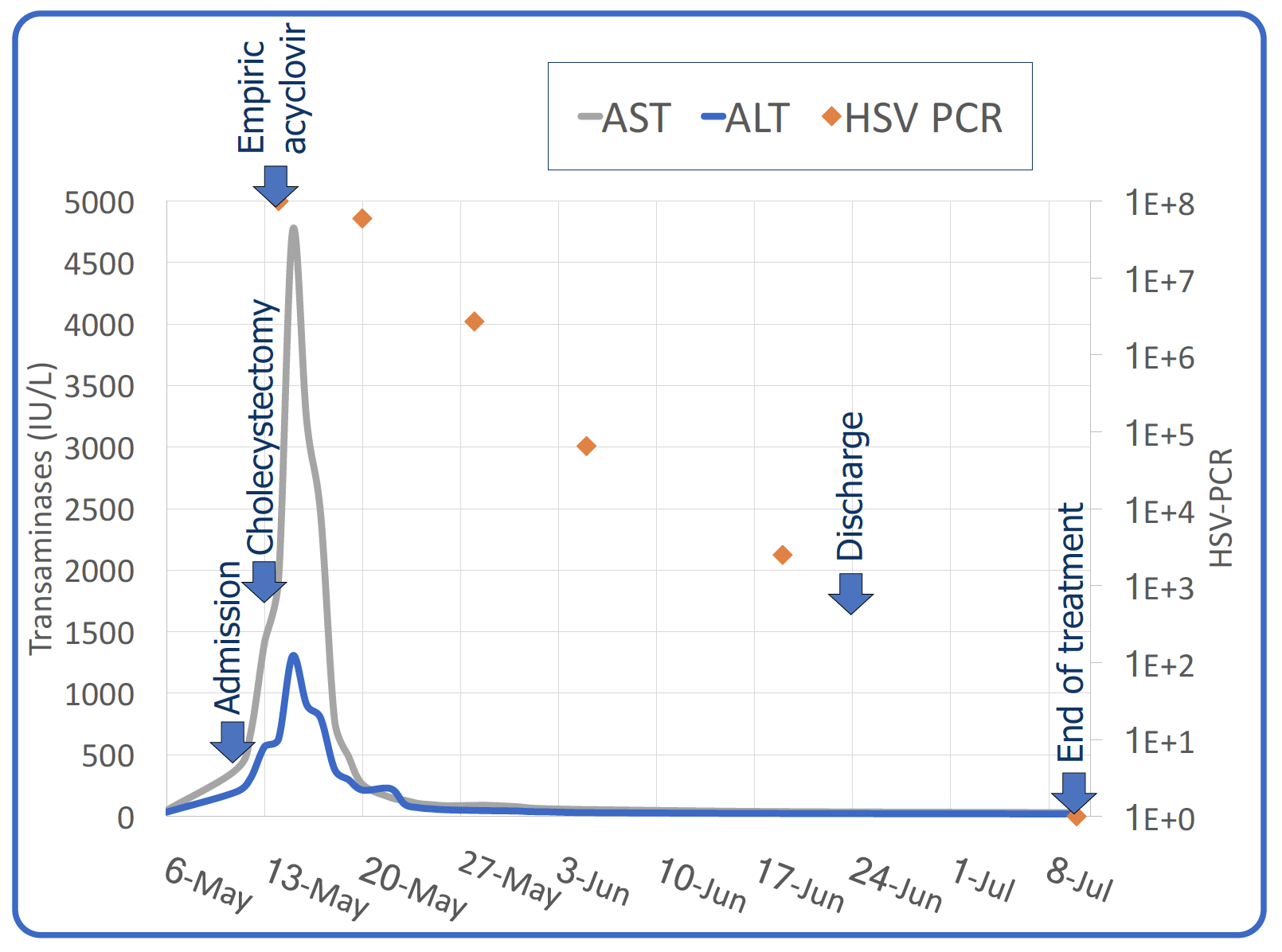
Despite delivery, she remained clinically unstable and her transaminitis worsened (AST:1986, ALT:662). Herpes simplex virus (HSV) hepatitis was suspected, and acyclovir was initiated. A serum HSV PCR returned positive at >1×10^8 copies/mL. The remainder of her infectious and autoimmune workup was negative. She clinically improved on acyclovir, corresponding to rapid improvement in her viremia. She was discharged home on day 29 to complete 6 weeks of IV acyclovir followed by 8 additional weeks of valacyclovir. Her daughter was empirically treated and had an uncomplicated postnatal course.
Discussion: Although HSV hepatitis is more commonly seen in neonates, both HSV 1 and 2 can cause acute hepatitis. Almost all adult cases occur in immunocompromised states including pregnancy, possibly due to physiologic hemodilution of IgG. Instead of fulminant hepatic failure, HSV hepatitis typically presents as severe sepsis and only half of patients have cutaneous or mucosal herpetic lesions. As in this case, the diagnosis is often elusive and with an untreated mortality rate of nearly 90%, three-fourths of case are diagnosed post-mortem. Definitive diagnosis can be made with hepatic biopsy, but in patients who are unable to undergo biopsy, early empiric antiviral therapy is crucial. Treatment with acyclovir can reduce mortality rates by more than 50%. Treatment duration is not well defined, though most case reports gave at least 2 weeks of acyclovir, or assured resolution of viremia. Liver transplant is indicated for patients with fulminant hepatic failure.
Conclusions: HSV hepatitis is a rare but devastating disease affecting mostly neonates and immunocompromised adults. Hospitalists need to be aware of this clinical entity as early diagnosis and treatment are crucial for survival.