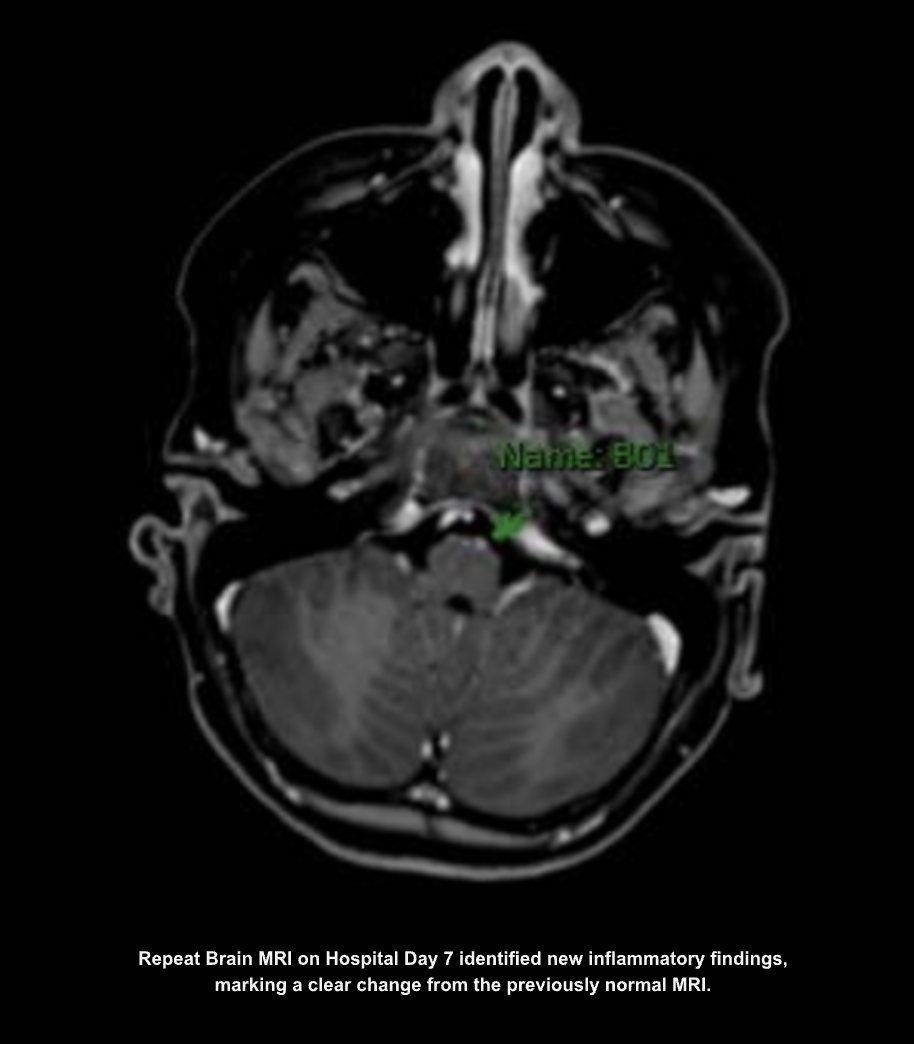
Case Presentation: An 11 year old male with chronic migraines presented with two weeks of worsening headaches, vomiting, poor intake, fever, fatigue, and fluctuating mental status. What initially resembled his usual migraines evolved into unrelenting daily headaches that no longer responded to home therapy. He developed new concerning features, including weakness in his legs, urinary symptoms, and brief episodes of hallucinations.ED evaluation raised concern for meningitis. Labs showed leukocytosis and elevated CRP. Lumbar puncture revealed a markedly elevated opening pressure and neutrophil-predominant pleocytosis, supporting presumed viral meningitis. Head CT was unremarkable. He was admitted and supportive therapy was initiated, but his fevers, headaches, weakness, and encephalopathy persisted. A repeat LP on hospital day five again showed neutrophilic pleocytosis, elevated intracranial pressure, and reduced CSF glucose, inconsistent with improving viral meningitis. Extensive infectious testing, including bacterial, viral, fungal, and metagenomic CSF studies, remained negative.As new hyperreflexia and diplopia concerning for CN VI palsy emerged, Neurology, Infectious Diseases, Ophthalmology, and Rheumatology were consulted. Subsequent MRI on hospital day seven demonstrated new inflammatory lesions in the cerebellum, medulla, and left optic nerve. In the setting of persistent encephalopathy, urinary symptoms, optic nerve involvement, and negative infectious workup, the leading diagnosis shifted to MOG antibody–associated disease (MOGAD). High-dose IV steroids were started which improved headaches, but hyperreflexia and urinary symptoms persisted leading to the initiation of IVIG.
Discussion: This case illustrates the evolving diagnostic complexity often encountered in hospital medicine. Although initial CSF findings suggested infectious meningitis, his clinical course diverged from expected improvement. Repeatedly negative infectious testing, worsening neurologic deficits, and development of double vision necessitated ongoing diagnostic reassessment and multidisciplinary collaboration. MOGAD is an inflammatory demyelinating condition that can mimic infectious meningitis, particularly when CSF demonstrates neutrophilic pleocytosis and elevated opening pressure.Recognition of this atypical presentation required continuous inpatient monitoring, repeated imaging and LPs, and coordinated consultations, highlighting the hospitalist’s critical role in navigating diagnostic uncertainty, integrating subspecialty input, and ensuring timely initiation of necessary therapies. This case demonstrates how rapidly evolving neuroinflammatory disease can present within a single hospitalization.
Conclusions: In pediatric patients with refractory headache, elevated intracranial pressure, and persistent pleocytosis, clinicians must consider autoimmune etiologies when infectious studies remain negative. This case demonstrates an unusual presentation of MOGAD mimicking meningitis and underscores the hospitalist’s role in navigating evolving diagnostic data and implementing early therapy.
.png)