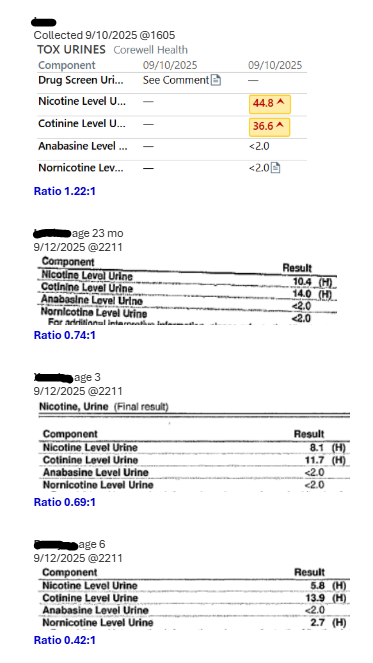
Case Presentation: 13-month-old male was found unresponsive and cyanotic in his crib at home by family members. Bystander CPR was initiated by family. Pulses palpated upon EMS arrival; rescue breathing initiated. Per history, his older brother had emptied a “drawer full of clothes” on him. No recent illness noted. On arrival to the ER, he was hypotensive, tachycardic & febrile. On exam he had a GCS of 4 with anisocoria. He was intubated and admitted to the PICU. Empirically, ceftriaxone and midazolam were administered for concerns of potential meningitis and subclinical seizure activity. CT was concerning for cerebral and cerebellar edema. Upon admission to PICU, he was found to have rhythmic jerks of hands, jaw, feet, and tongue. Loaded with levetiracetam, fosphenytoin, and phenobarbital while awaiting cEEG. EEG showed severe encephalopathy. Child advocacy team was consulted. On hospital day 2, patient had worsening intracranial hypertension. Repeat imaging confirmed progressive cerebral edema, loss of gray-white differentiation, and tonsillar herniation. Comprehensive urine drug screen was positive for nicotine and cotinine. The concentrations were much higher than expected for passive exposure, consistent with ingestion. Anabasine and nornicotine were negative. Simultaneously, bedside nurse reported that the patient had passed small white fiber packets in his stool along with expected mucosal sloughing. These pouches were not sent for toxicological analysis. It was noted that the patient’s family used flavored nicotine pouches and vape liquid at home. Patient’s condition progressed to brain death after clearance of his neuro-sedatives. While ingestion of nicotine pouch(es) cannot be confirmed, the concentration of nicotine suggests a potential contributor to his anoxic brain injury.
Discussion: Pediatric nicotine exposures can occur from many products besides cigarettes, including lozenges, flavored gums, liquids, tablets, and, more recently, oral nicotine pouches. These pouches, marketed under names like Zyn, have surged in popularity in the United States, with sales increasing 641% from 2019 to 2022 (1). With the increasing nationwide consumption of Zyns comes the elevated risk of accidental nicotine overdose among children. Symptoms range from mild tremor, increased salivation, nausea, and vomiting to life‑threatening cardiac arrhythmias, muscle fasciculations, seizures, and coma (2). Doses in the order of 6.5–13.0 mg/kg body weight can be fatal for children (3). A recent analysis of unintentional nicotine ingestions in US children younger than six years identified 134,663 cases; 98.5% occurred at home, and the majority occurred in children < 2 years of age (4). Flavored nicotine pouches in brightly colored packaging are particularly hazardous because they attract young children and can mask nicotine’s taste and odor. When toxin ingestion is suspected, include nicotine and its metabolites in the toxicology workup. Common analytes include nicotine, cotinine, norcotinine, anatabine, and anabasine; anabasine and anatabine help distinguish tobacco‑derived exposures from non‑tobacco nicotine products (5,6). In our case, the specimen contained nicotine and cotinine but lacked anabasine, suggesting ingestion of a non‑tobacco nicotine formulation such as a nicotine pouch.
Conclusions: Nicotine pouch and e-cigarette use is skyrocketing in the United States, and it is important to understand that they present a significant threat of overdose among children, particularly toddlers.