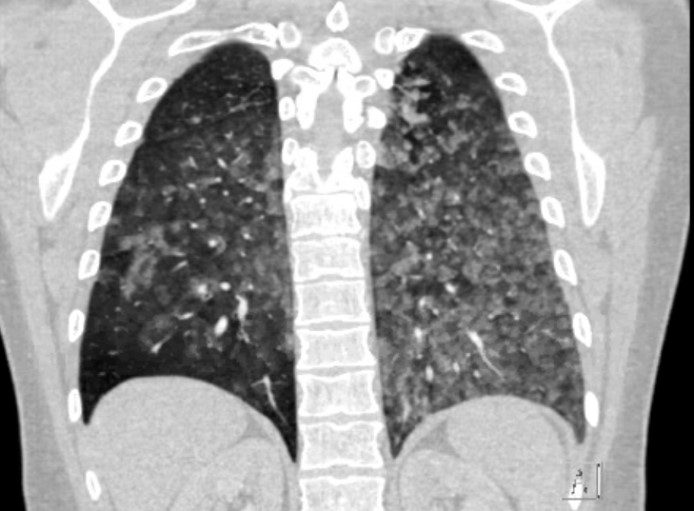
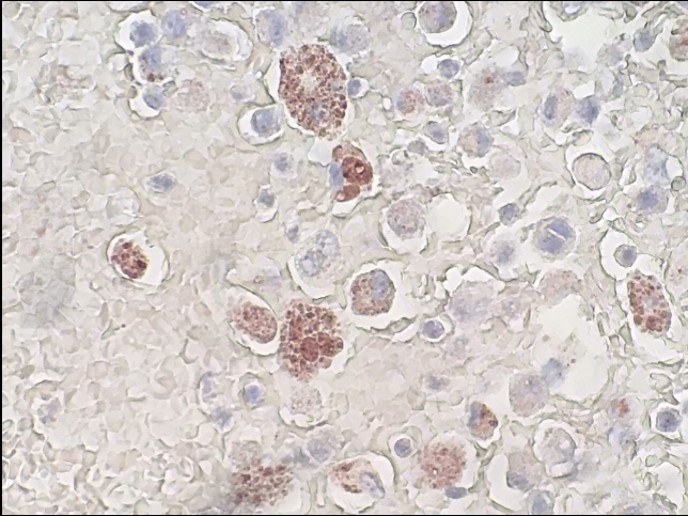
Case Presentation: A 24 year-old man with past medical history significant for tobacco, marijuana, and e-cigarette use presented to the emergency department for hemoptysis, dyspnea, cough with pleuritic chest pain, and subjective fevers. Twenty-four hours prior to presentation, the patient endorsed first-time use of a street-purchased e-cigarette cartridge containing tetrahydrocannabinol (THC). The patient had acute hypoxic respiratory failure with an oxygen saturation of 90%, but was otherwise hemodynamically stable. Physical exam was notable for diffuse expiratory crackles. Urine drug screen was positive for cannabinoids and THC. Laboratory testing demonstrated a leukocytosis of 29,700/µL with a neutrophil predominance and a hemoglobin of 12.7 g/dL. Infectious work-up with blood and sputum cultures, legionella and pneumococcus antigens, and HIV antibodies was negative. Inflammatory markers (ESR, CRP) and autoimmune markers (ANA, ANCA) were unremarkable. CT imaging of the lungs demonstrated diffuse ground glass nodular opacities in the upper and lower lobes bilaterally. Bronchoscopy was performed and cytology of bronchiolar lavage revealed lipid laden macrophages with oil red O staining characteristic of lipoid pneumonia. The patient was treated with IV methylpredinsone with resolution of the leukocytosis, normocytic anemia, and bilateral opacities on chest x-ray. He was discharged on a 5-day taper of oral prednisone and counseled on cessation of e-cigarette products.
Discussion: E-cigarette use has increased in prevalence with the highest rates of current and regular use in persons aged 18-24 years. Most patients with e-cigarette and vaping-associated lung injury (EVALI) present with respiratory distress, nausea, vomiting, abdominal pain, diarrhea, and fever within 2-3 months of initiation of use. EVALI can present in a variety of ways including lipoid pneumonia, hypersensitivity pneumonitis, diffuse alveolar hemorrhage, and acute eosinophilic pneumonia. The proposed mechanism of lung injury in lipoid pneumonia is heating of the e-cigarette cartridge leading to aerosolization of oils (commonly vegetable glycerin) which deposit within the alveoli and cause an inflammatory response. The diffuse ground glass opacities on CT demonstrate diffuse deposition from vaping rather than basilar distribution associated with aspiration. Approximately 80-90% of EVALI cases have been associated with the use of THC-containing products. Unlike e-cigarette nicotine-products, THC-products are often street-purchased and contain unknown substances. Treatment of lipoid pneumonia is aimed at discontinuation of the offending agent. The efficacy of corticosteroids for treatment is unclear. However, other cases of vaping-associated lipoid pneumonia demonstrated clinical improvement after IV corticosteroids.
Conclusions: Our case represents a 24 year-old man presenting with acute lipoid pneumonia due to vaping a THC-product. EVALI presents with nonspecific symptoms, but physicians must recognize its increasing incidence with the expanding use of street-purchased e-cigarette cartridges containing THC and other unknown components. In EVALI cases, we recommend obtaining the offending e-cigarette cartridge for composition analysis.