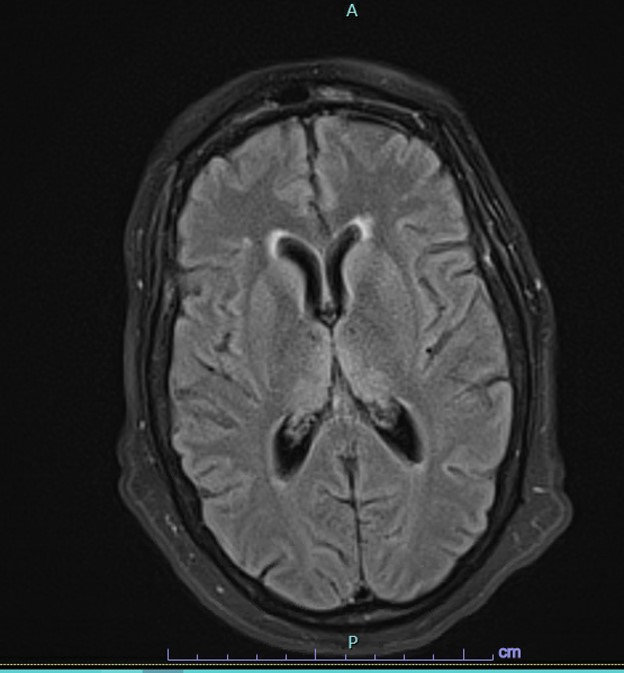
Case Presentation: A 53-year-old female with a history of hypertension presented with encephalopathy. 2 days prior, her family noticed that she was making bizarre statements that did not correlate with reality. Notably, she had a positive COVID-19 test 3 weeks prior. Social history was significant for consumption of 100-125 ounces of beer per day and occasional marijuana use. Physical exam revealed orientation only to self, visual hallucinations, gait ataxia, and confabulations. Labs were largely unremarkable, except for lymphopenia, calcium 12.6, PTH 170.2, and protein gap 5.2. Urine drug screen was negative. Blood cultures were positive for Staphylococcus warneri. Initial CT head and MRI brain were negative. The patient was treated with culture-directed antimicrobials, high-dose thiamine, and zoledronic acid without improvement in her encephalopathy. Further workup, including autoimmune studies, paraneoplastic panel, continuous EEG, and serum protein electrophoresis, was unrevealing. Lumbar puncture (LP) was positive only for Acinetobacter radioresistens in cultures. She was treated with appropriate antibiotics for 3 weeks, and repeat LP was negative. Repeat MRI brain showed a nonspecific rind of periventricular white matter FLAIR and hyperintensities in the medial thalami. A diagnosis of Wernicke-Korsakoff syndrome was made, and the patient was ultimately discharged to a skilled nursing facility.
Discussion: Wernicke-Korsakoff syndrome is a combination of two separate conditions, Wernicke encephalopathy (WE) and Korsakoff syndrome (KS), and is the most well-known neurologic complication of thiamine deficiency. It is classically seen in patients with prolonged alcohol use. WE is an acute syndrome manifested by the classic triad of encephalopathy, oculomotor dysfunction, and gait ataxia. KS is a chronic neurologic disorder that occurs as a result of WE and often presents with anterograde and retrograde amnesia.[1] Our patient had a positive COVID-19 test 3 weeks prior to presentation, which caused her to self-isolate. Her mental status deteriorated during this isolation, the timeframe of which is unknown. The most reasonable explanation is that she developed WE that then progressed to KS before she was able to be treated with high-dose thiamine.However, given the unknowns of COVID-19, COVID-19 associated encephalopathy must be considered. Prolonged encephalopathy is an emerging complication of COVID-19 that is most commonly seen in patients over age 50. It typically presents with altered mental status (ranging from mild confusion to deep coma) preceded by more common manifestations of COVID-19 infection, such as fever, cough, and dyspnea.[2] The pathogenesis is multifactorial and includes inflammatory, metabolic, and hypoxic processes.[3] Neuroimaging is normal in most patients but may show periventricular signal changes, such as those seen in our patient.[2] Most patients improve without long-term sequelae. However, there have been reports of prolonged encephalopathy months after initial diagnosis, although this may be more common in those who are critically ill.[4] Continued investigation is required to fully delineate the effect of COVID-19 on the nervous system.
Conclusions: Encephalopathy is one of the most common complaints a physician will encounter. Due to increasing prevalence of COVID-19, COVID-19 associated encephalopathy must be considered in all patients with a reported history of infection.