
Background:
Venous thromboembolism, unstable angina, and atrial fibrillation are diseases that utilize parenteral anticoagulant therapy, which is often associated with bleeding and thrombocytopenia that require management and a prolonged hospital stay and pose an economic burden to the health care system. Historically, unfractionated heparin (UFH) is preferred because of the low acquisition costs of UFH compared to low‐molecular‐weight heparin (LMWH). Experts have long debated whether overall costs should drive pharmacy choices for drugs. Studies evaluating UFH and LMWHs have shown a difference in efficacy, but none has actuaily evaluated differences in overall charges to the health system and safety (bleeding, thrombocytopenia, and transfusion requirements) across 3 medical conditions. We sought to compare health care charges, length of stay (LOS), and the rate of adverse events between UFH and LMWH.
Methods:
We designed a retrospective cohort study at an academic medical care center between January and September 2008 to include all patients who received therapeutic doses of UFH or LMWH. We collected baseline demographic data and medical comor‐bidities by crosslinking the pharmacy, administrative, and billing databases. Patients were included only once. Outcomes were defined using the ICD‐9 codes and included gastrointestinal bleeding, subarachnoid hemorrhage, thrombocytopenia, and transfusion requirements. Other outcomes included LOS and 30‐day readmission, and finally hospital charges for the admission were also collected. For baseline characteristics we used the chi‐square and t tests. To determine the adjusted mean of costs and LOS, we used generalized linear models. To determine the rate of categorical events, we used logistic regression.
Results:
There were a total of 647 patients who received LMWH and 258 that received UFH. Other baseline characteristics are shown in Table 1. Overall, after adjustment for age, sex, and the Charlson score, the mean adjusted hospital charges were significantly iower with LMWH ($66,843, Cl $61,629–$72,057, P < 0.01) compared with UMH ($105,127, Cl $96,617–$113,637). The median adjusted length of stay (LOS) was also significantly lower in the LMWH group (7.9 days, Cl 7.2–8.6 days, P < 0.01) compared with UFH (12.1 days, Cl 10.9–13.2 days). The 30‐day readmission rate was 0.07 (Cl 0.05–0.09, P < 0.01) compared with UFH (0.02, Cl 0.0–0.05). The odds ratio (OR) for gastrointestinal bleeding for LMWH compared with UFH was 0.30 (Cl 0.12–0.72, P < 0.01). Subarachnoid hemorrhage and thrombocytopenia rates did not differ between the 2 groups. The adjusted OR for transfusion needs for LMWH compared with UFH was 0.71 (Cl 0.48–1.04, P = 0.05).
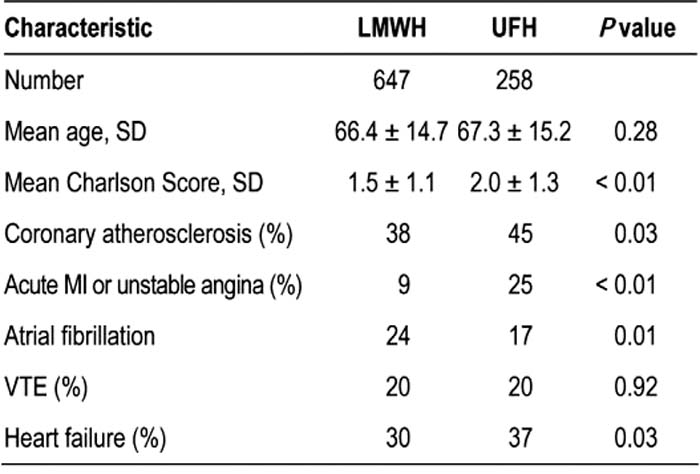
Table 1. Baseline Characteristics
Conclusions:
LMWH use is associated with lower health care charges, lower LOS, and increased safety related to bleeding compared to UFH. There is a minimal increase in the 30‐day readmission rate with LMWH. These findings have implications for clinicians when selecting a parenteral heparin to treat a condition or for nonclinicians when making a formulary choice.
Author Disclosure:
A. Jaffer, sanofi‐aventis, consultant and speakers bureau; Astra Zeneca, consultant; SPAQI, AF Forum, board member; L. Magras, none; W. O'Neill, none; L. Tamariz, none; Y. Yang, none.