Background: Our healthcare institution serves a large low-income, minority, and historically underserved population. The shortage of primary care physicians (PCPs) in our city and the high complexity of patients that are cared for by our organization is a challenge. Patients are in need of transitional care our institution and need help to connect to other in-network PCPs. The partnership between Hospitalists and PCP’s to provide transitional care at the right time and under specific core aims is essential for the patient’s safety, quality of care, and outcomes.
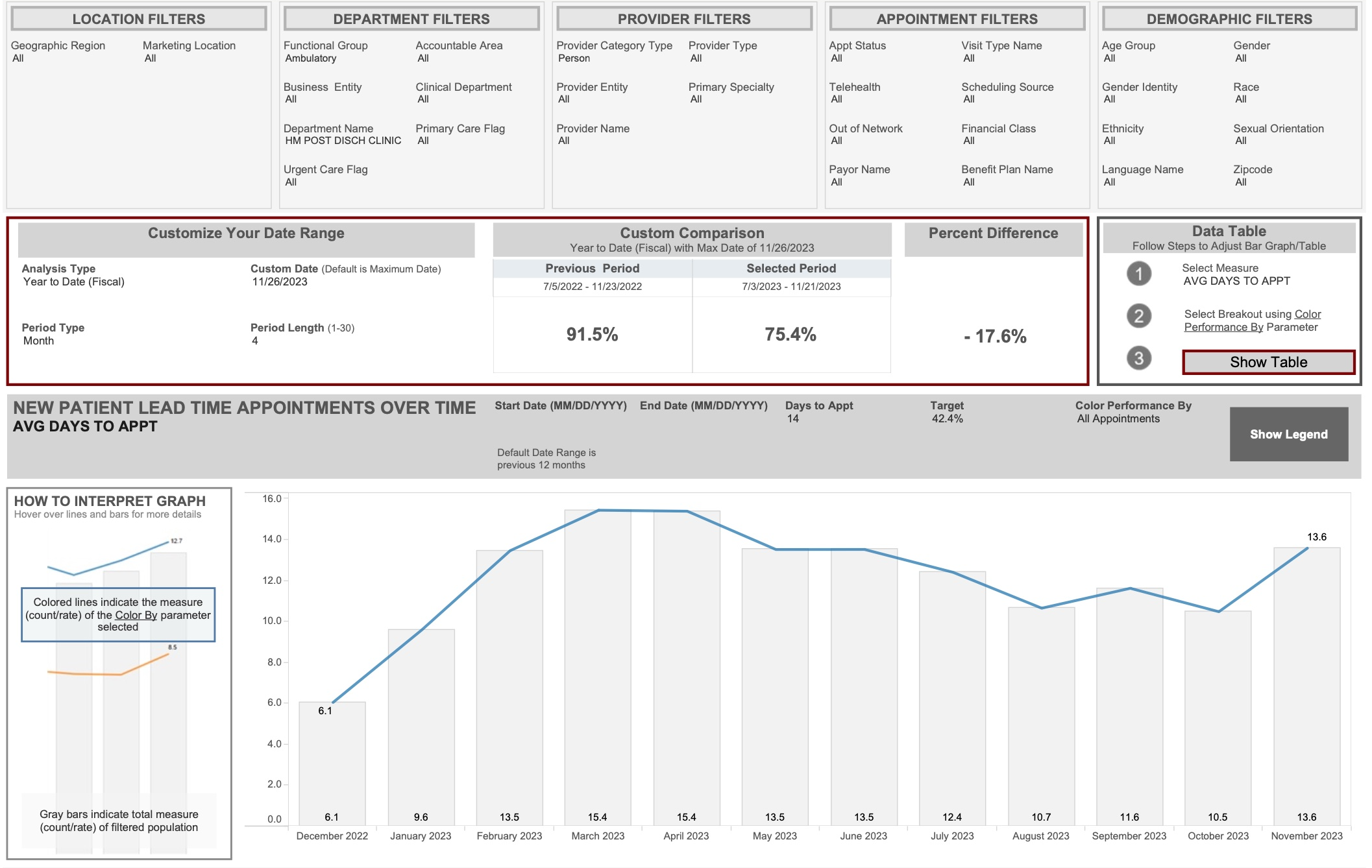
Purpose: Our post-discharge clinic (PDC) implements transitional care initiatives to address the needs of patients, hospitalists, and primary care physicians (PCPs) to improve ambulatory care access within 14 days post-discharge, and to improve quality of care and operational efficiency.
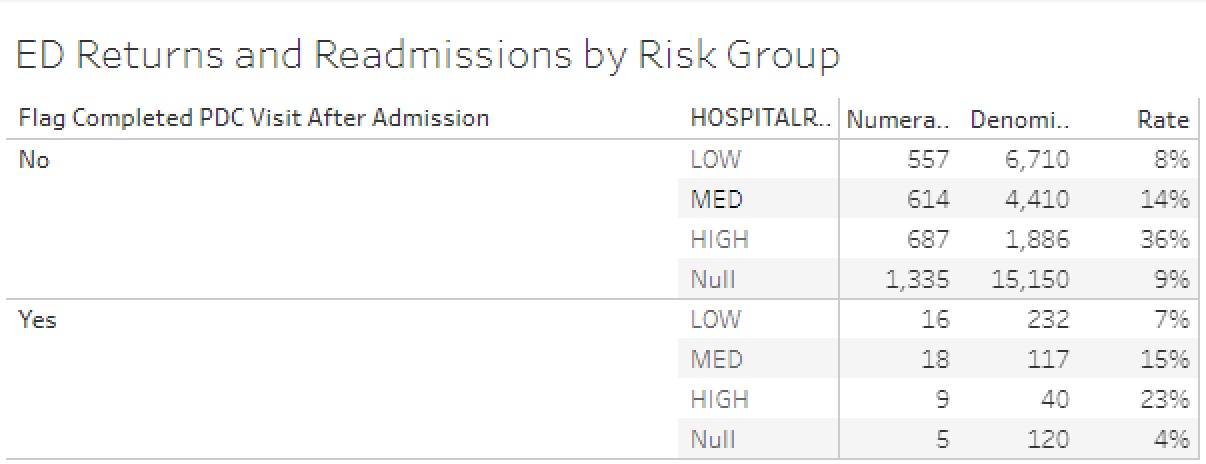
Description: We established a hybrid clinic that provides virtual and in-person visits. We stratified patients according to the risk of readmissions (ROR). We schedule patients based on their ROR, thus inferring how sick the patients are, and consider if they need to be seen virtually or in person. That appointment is scheduled before patients leave the hospital. Forty-eight hours after hospitalization, patients receive a call from the transitional care nurse to obtain information about the patient’s clinical status and to answer any questions patients may have. That note is documented in the electronic medical record as a transitional care management call and any urgent issues are addressed on the call. Sicker patients are scheduled within 7 days post-discharge and leadership prefers in-person visits. Otherwise, patients with low and moderate ROR are scheduled within 14 days of discharge. During the visit, we provide the patient and their family with education about their medical conditions, perform medication reconciliation, identify possible adverse events, provide a positive experience for patient’s and family members, and reinforce the needs of short- and long-term medical adherence. The PDC provides 100% access for patients who need to see a PCP within 14 days of hospitalization and our average/median days to the next new appointment is 14.2/12.0. The PDC provides a flexible open schedule for sicker patients in need of in-person or close follow up within 7 days post-hospitalization. Patients seen at the PDC maintain open communication with PCPs electronically through EPIC, secure chats or phone calls, and coordinate transitional support with internal and external stakeholders. Our quality is measure by the rate of readmissions. Patients seen at the PDC have 33% less readmissions that patients not seen at the PDC.
Conclusions: Our transitional innovation improves post-hospitalization primary care access and enhances patient safety and quality of care, especially in patients with higher ROR. Larger sample for patients with higher ROR may be needed for statistical significance.