Background: Medically acute patient patients are cared for by housestaff and advance practice provider (APPs) overnight. The severity of illness in these patients can vary during their hospital stay. Decompensation in this population is under recognized and can lead to adverse outcomes. Even when correctly identifying decompensation, unclear lines of escalation, and poor documentation practices can lead to suboptimal outcomes.
Purpose: The target for this intervention is DIOs, program directors, service chiefs and housestaff and APPs who care for patients overnight. The goal of this program is to create a framework to support housestaff and APPs in identifying decompensating patients during overnight shifts. When these patients are identified, this framework establishes clear lines of escalation, and supports clear and concise documentation.
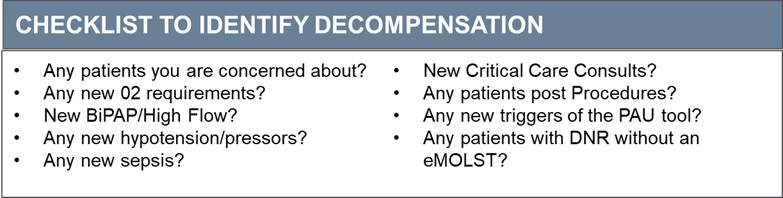
Description: This three part intervention targets identification of decompensating patients, support for improved documentation and a clear plan for escalation. To improve identification of decompensating patients, we created a checklist of indications placing patients at high risk of decompensation (Fig 1). During nightly Hot Spot rounds, the newly-created Team Captain hospitalist meets with each team of housestaff or APPs and uses the checklist to identify patients at risk of decompensation. Additional patients were identified by the use of an automated predictive analytic built into the electronic medical record system. These patients are then seen together at the bedside with the hospitalist. In order to support documentation, we created a template note that encouraged clear and concise documentation with contingency planning (Fig. 2). We recorded the number and frequency of identification of hotspot patients. Hotspot notes were graded on a 5-item rubric for the absence or presence of Clarity, Contingency planning, Concision, Clinical Assessment, and Communication.In the first three weeks of implementation, 84 patients were identified as hot spots, with 2-7 identified each night. This was a sick group of patients, with 16 (19%) requiring rapid response or transfer to the ICU within 24 hours. The most common cause for a hotspot was sepsis (21%) followed by respiratory distress (17%). Of patients identified as Hot Spots, 70 (83%) had a note written by the overnight housestaff or APP. 49 notes were written using the Hotspot template. Notes using the template were highly rated on Clarity, Clinical Assessment, Concision and Communication. Contingency planning was rated poorly (Fig 3).
Conclusions: Implementation of this three part intervention identified decompensating patients overnight, created a clear line of escalation, and created a note template that supported documentation that was rated highly for clarity, communication, concision, and clinical assessment. Implementation of this program will support housestaff and APPs in identifying decompensating patients. Next steps include expansion to other services and better integration of the electronic medical records automated decompensation warnings.