Case Presentation:
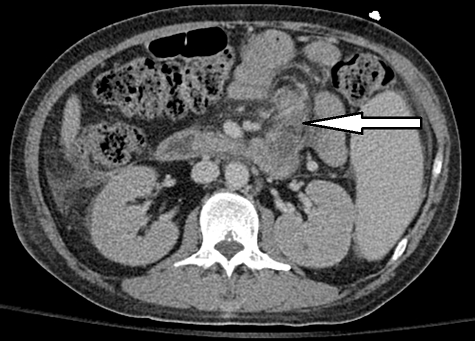
A 37-year-old man with AIDS on HAART and chronic therapy for history of mycobacterium avium infection (MAI) presented with altered mental status 4 weeks after stopping his medications. Family reported progressive confusion and weight loss. On physical examination his temperature was 38.1°C , blood pressure 130/50, heart rate 118, respiratory rate 16 with O2 saturation 95% on room air. He was somnolent, cachectic and had no focal findings on exam. Labs showed normocytic anemia 8 gm/dL, leukopenia 0.9 /uL thrombocytopenia 60 /uL, CD4 count 7/mm3, creatinine 1.4 mg/dL, corrected Ca 12 mg/dL, PO4 2 mg/dL , ionized Ca 1.6 mmol/L and albumin 1.8 g/dL. He was given fluids for hypercalcemia and restarted clarithromycin and ethambutol for MAI but corrected serum Ca trended up slowly to 14 mg/dl by day 6 so calcitonin was given for 3 days with pamidronate with normalization of serum calcium and improvement in the patient’s mental status. Further work up included Vitamin D was 5 ng/dL, low PTH 6 pg/ml and PTHrp was undetectable. Brain MRI showed small scattered areas of abnormal parenchymal signal intensity likely from infectious meningoencephalitis. CT of the chest, abdomen and pelvis revealed necrotic mesenteric lymph nodes and splenomegaly. Serum protein electrophoresis and skeletal survey were negative. Bone marrow biopsy revealed bone marrow infiltration by granulomas positive for acid fast bacilli and cultures grew MAI. Final diagnosis was disseminated MAI with resultant hypercalcemia that worsened with initiation of MAI therapy.
Discussion:
The mechanism of hypercalcemia in granulomatous disease may be related to vitamin D dysregulation but does not always correlate with vitamin D metabolite levels. Two cases in the literature presented with MAI and hypercalcemia while four other cases reported hypercalcemia after weeks of initiating treatment for MAI. Vitamin D metabolites were not all elevated in those reports. Our patient both presented with hypercalcemia which worsened within days of restarting MAI therapy. Given his level of hypercalcemia and pancytopenia, steroids were not given and an extensive work up for malignancy was performed. The clue to the diagnosis was necrotic lymph nodes on axial imaging. Treatment with calcitonin and pamidronate was effective.
Conclusions:
Hypercalcemia>13 mg/dL in the hospitalized patients is often attributed to malignancy but patients with HIV warrant investigation into opportunistic infections such as MAI. Hypercalcemia from MAI can be treated with calcitonin and pamidronate.