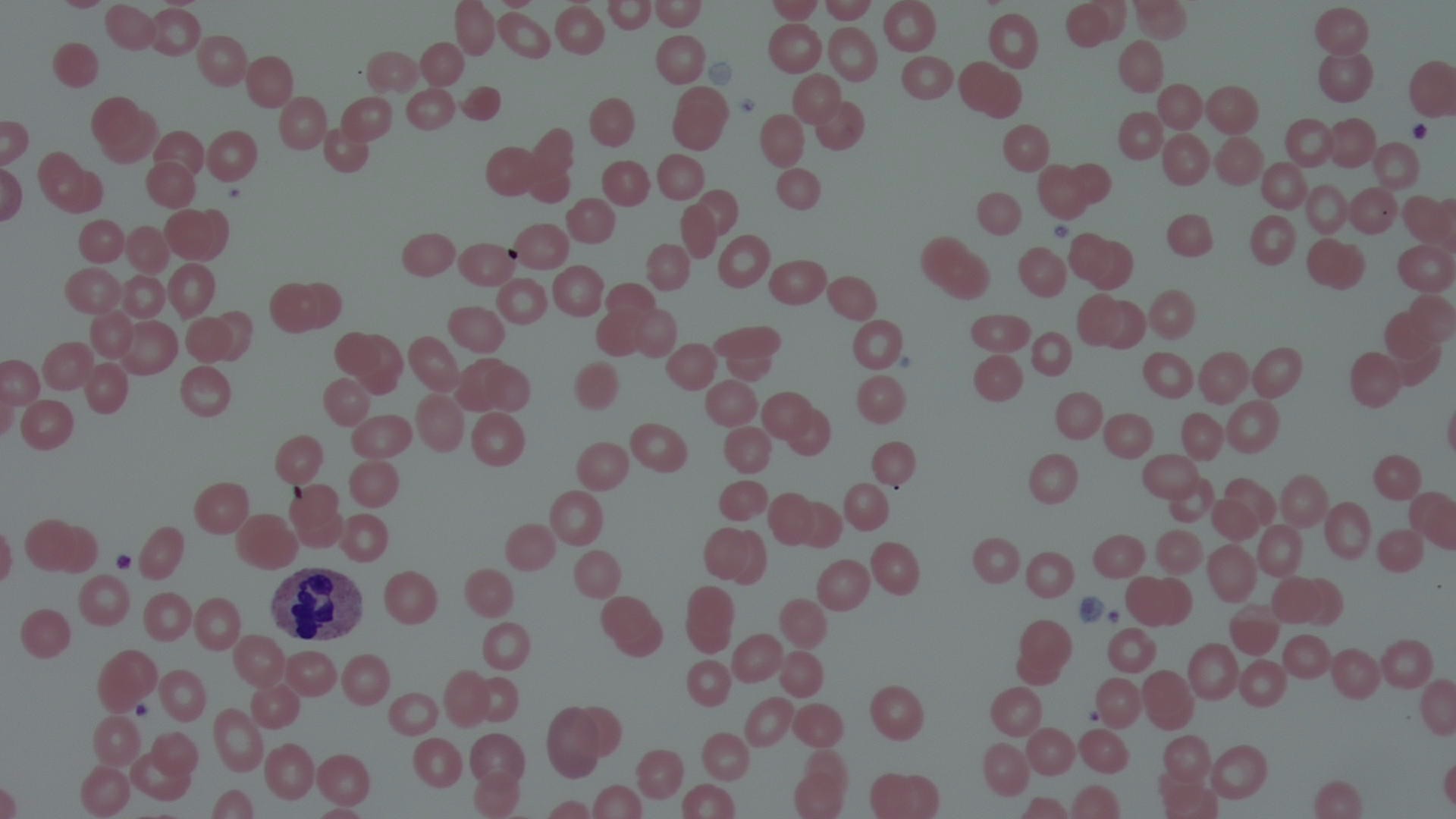
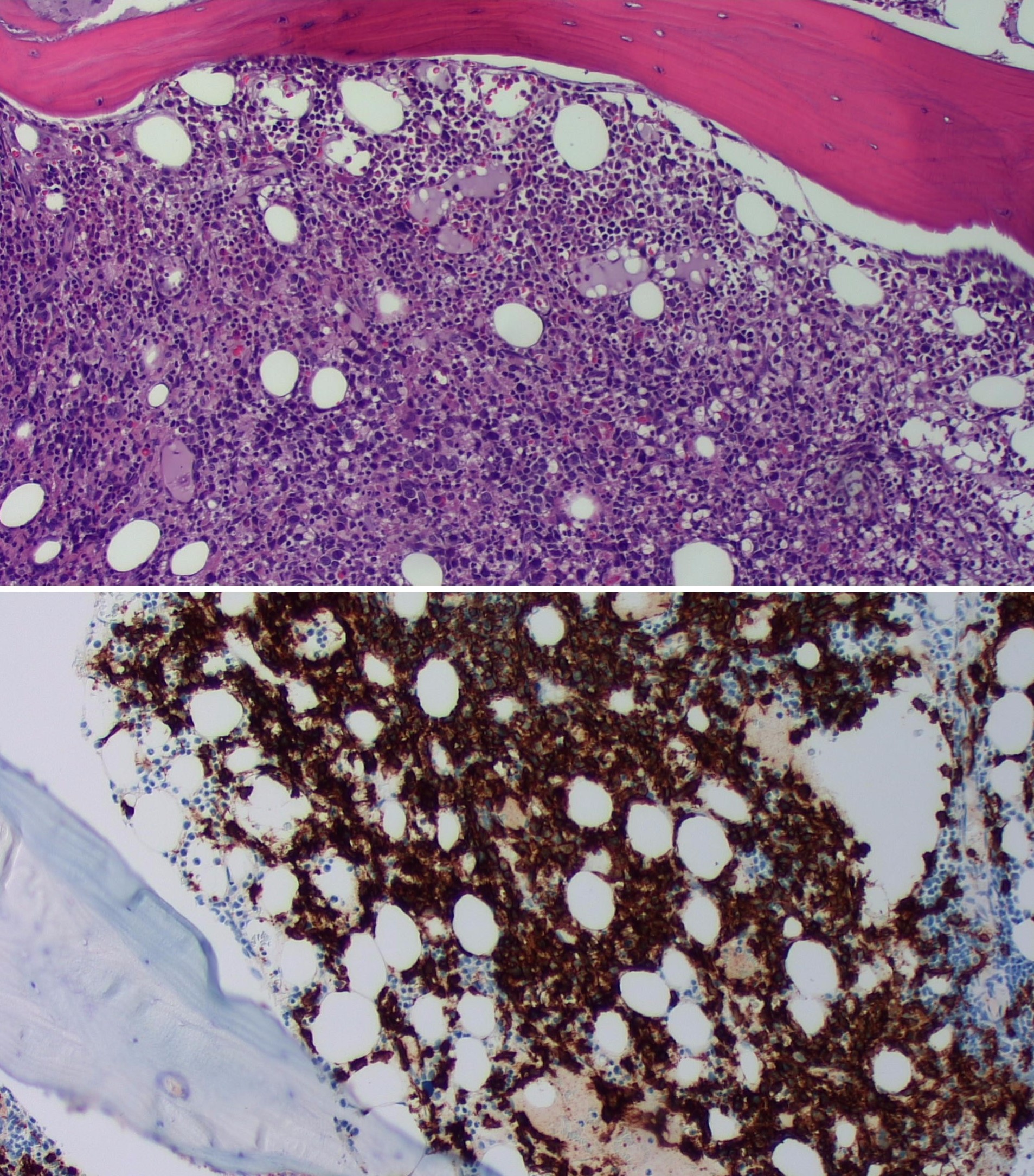
Case Presentation: 78 y/o M with past medical history of Diabetes Mellitus type 2, Dyslipidemia ,RCC s/p partial nephrectomy presented with altered mental status. Symptoms started with fatigue, generalized weakness, SOB, 18-20 pound weight loss, constipation ,loss of appetite and confusion that started 1 month ago. Patient appeared frail, was not oriented to time, place or person and was not following commands, no lymphadenopathy or organomegaly present. Basic labs were ordered and the only thing that stood out was hypercalcemia with a calcium level of 15.8. CT head was unremarkable. Diverticulosis and Low-density lesions in the spleen which may indicate underlying lymphoma or other tumor, infectious or inflammatory process, sequela of granulomatous disease on CT abdomen. Mild reticular airspace disease in the left lingula and dependent aspect of the lower lobes bilaterally, likely atelectasis or scarring on CT chest. PTH , PTHrP, 25 Hydroxyvitamin D, TSH all of which were low except 1,25dihydroxyvitamin D which was normal ,slightly elevated kappa light chain. Differentials included MM and hypercalcemia due to immobility. Treatment for hypercalcemia initiated with IV fluids, calcitonin, and zoledronic acid. After 3 days, his hemoglobin started to drop. Labs showed normocytic anemia, no signs of bleeding, ferritin 1416, low iron levels. LDH and haptoglobin elevated. Peripheral blood smear showed pancytopenia with lymphopenia with reactive changes, granulocytes with reactive changes (hypergranulation and vacuoles), normocytic anemia with no specific RBC morphologic abnormalities, thrombocytopenia of unknown etiology, and no blasts or dysplastic changes were identified. This was concerning for hematological malignancy with multiple myeloma high in the differentials. A bone scan was done which showed symmetrically increased periarticular radiotracer accumulation in association with bilateral knees and ankles. A bone biopsy was done and showed malignant B-cell lymphoma, multifocal and diffuse infiltration in the bone marrow with atypical lymphoid cells are B cells positive for CD20 and CD79a. A diagnosis of diffuse large B cell lymphoma was made.
Discussion: Our case was unique because this was an acute onset with atypical symptoms of Altered mental status, no lymphadenopathy and no masses were found on imaging. DLBCL usually presents as a Rapidly enlarging symptomatic mass with Systemic “B” symptoms observed in approximately 30 percent of patients, and the serum lactate dehydrogenase (LDH) is elevated in over one-half. Bone marrow is involved in up to 30 percent of cases. Diagnosis is best made based on excisional tissue biopsy, however in our case a bone biopsy was diagnostic. Hypercalcemia is mostly secondary to increase in 1,25 dihydroxy vitamin D. In our patient 1,25 dihydroxy vitamin D was also normal probably because the treatment for hypercalcemia was started before sending the labs out.
Conclusions: Hypercalcemia is a very commonly dealt situation, however when there are any concerns for malignancy (like weight loss, calcium level >13) more invasive methods can be used to diagnose the underlying pathology. In our patient, even hypercalcemia due to immobility was high in differential, however, given the patient was having weight loss and had a calcium level of 15, it was reasonable to completely rule out malignancy. Early detection of cancers like DLBCL can improve long term prognosis in such patients. Our patient currently has finished chemotherapy with CHOP R regimen and is in remission.