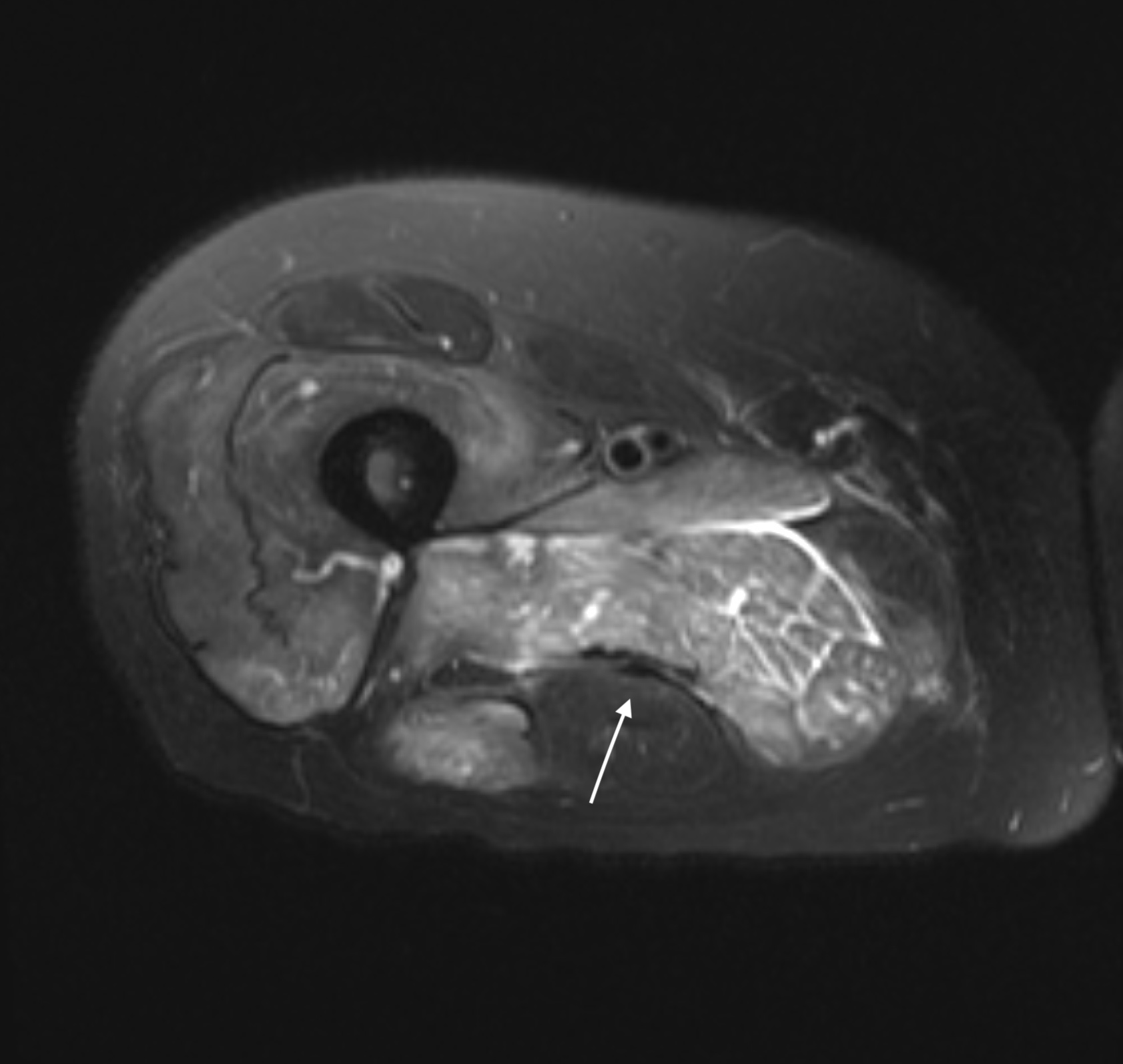
Case Presentation: A 65-year old woman taking a stable dose of high-intensity rosuvastatin presenting with 3 weeks of proximal extremity weakness and pain, noted to have an elevated creatinine kinase (CK) on presentation (7,459 U/L). Despite discontinuation of rosuvastatin and standard rhabdomyolysis management, CK levels failed to normalize, and patient continued noting persistent proximal muscle weakness, prompting additional work up. MRI of upper leg was completed noting nonspecific myositis, and muscle biopsy obtained noting non-specific inflammation, though results were limited due to sample collection. Immunosuppression was initiated empirically for autoimmune myositis per rheumatology with oral Prednisone. Following initiation of Prednisone, in addition to standard IV hydration, CK levels and muscle pain improved over 10 days, with intravenous immunoglobin (IVIG) also initiated for assistance in controlling CK levels. CK levels at discharge were elevated but improved (2,484), and muscle weakness was persistent but improving. Patient was discharged to inpatient rebab with Rheumatology follow up. Subsequent serology for Anti-HMG-Co-A reductase antibody (anti-3-hydroxy-3-methylglutaryl-coenzyme A reductase), a diagnostic marker of statin-induced immune-mediated necrotizing myopathy, resulted positive (516.80 CU; ref < 20.0), establishing diagnosis.
Discussion: This case highlights the clinical presentation of statin-induced immune-mediated necrotizing myopathy, an uncommon complication of statin use characterized by by statin-induced autoantibodies against HMG-Co-A reductase. Clinical features that should raise suspicion include proximal muscle weakness, elevated CK, and persistence of muscle damage even after discontinuation of statins. Presentation can occur in patients despite chronic use and prior toleration of statins. High suspicion in this scenario should prompt confirmatory diagnostic test including anti-HMG-Co-A reductase serology and muscle biopsy. Standardized immunosuppressive regimens have not yet been established, but initial treatment generally includes steroids and depending on response additional agents including IVIG, methotrexate, or rituximab. Prognosis varies, with some patients requiring long-term immunosuppression due to persistent or relapsing symptoms.
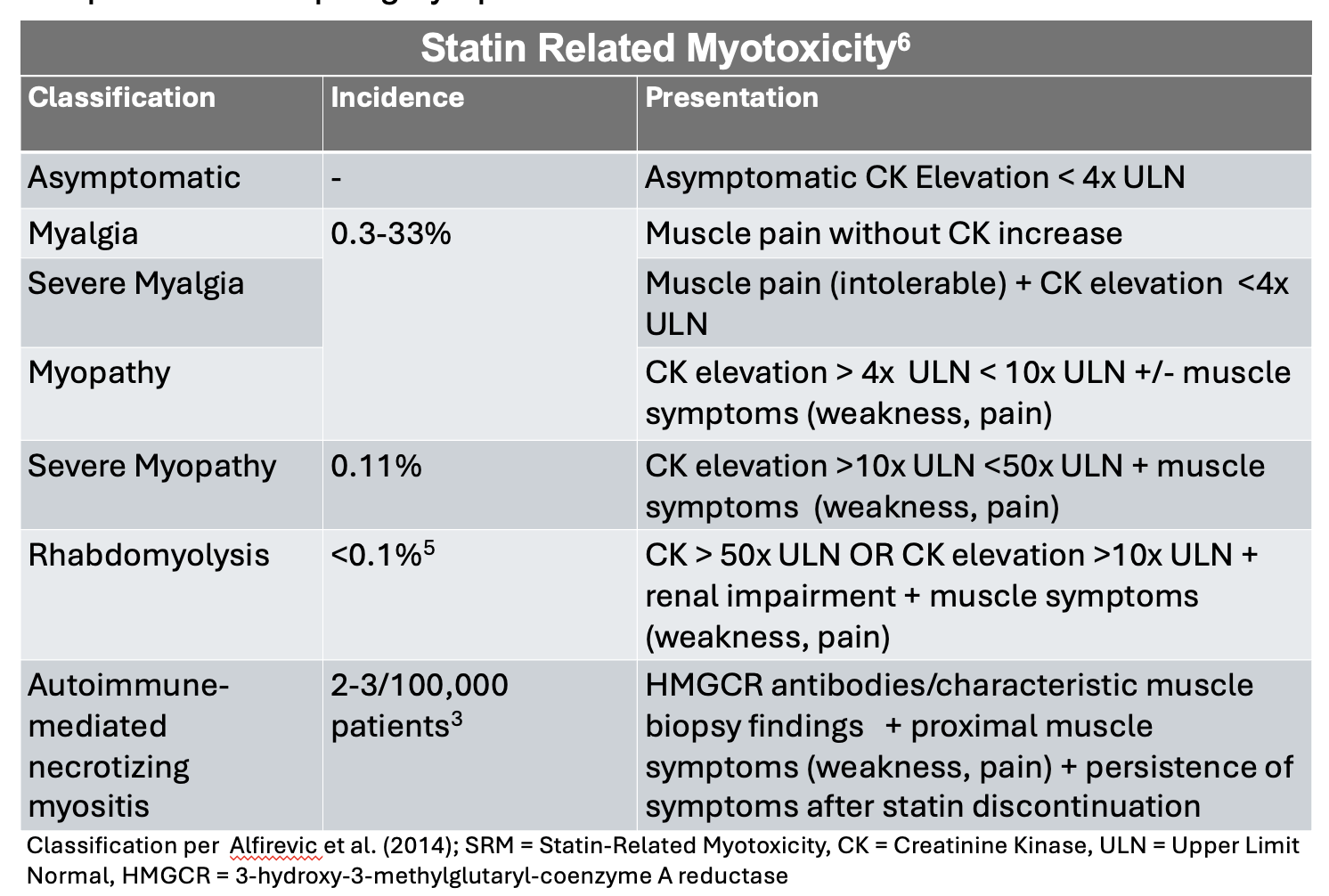
Conclusions: Statin-induced myopathy can occur on a spectrum ranging from benign myalgias to rhabdomyolysis; a rare auto-immune complication of statin use is immune-mediated necrotizing myopathy. Timely recognition of statin-induced immune-mediated necrotizing myopathy from other self-limiting forms of statin related muscle disease is essential as management is distinct, requiring immunosuppression to minimize disease progression and muscle damage.