Background: Medicine procedure services (MPS) have been shown to increase procedure volume, procedure completion rate, adherence to best practice safety measures, resident involvement, and resident satisfaction within Internal Medicine (IM). Despite these benefits, widespread deployment of MPSs has proved challenging, partly because the impact of MPSs on non-IM services is unknown, including MPSs’ impact on Interventional Radiology (IR) procedure volumes.
Purpose: As part of a process improvement project focused on reducing IR utilization to improve IR overcrowding and throughput at a large, resource-constrained academic medical center, we assessed our MPS’s impact on direct-to-IR referrals for common bedside procedures, including central venous lines (CVL), lumbar puncture (LP), paracentesis, and thoracentesis.
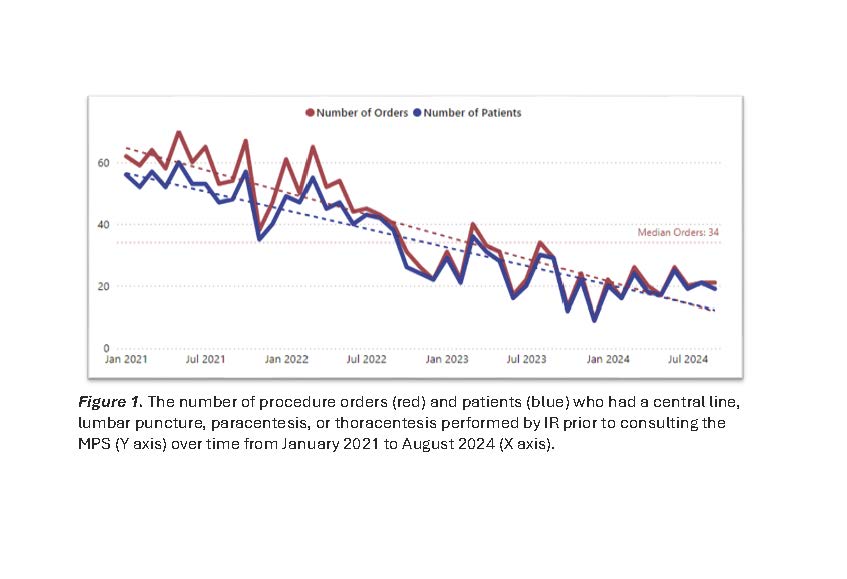
Description: In July 2020, the Division of Hospital Medicine launched an MPS offering common bedside procedures to inpatients hospital wide. In January 2021, we began tracking the number of inpatient procedures that were performed by IR without first involving the MPS, defined as the presence of an IR procedure order without an MPS consult order. In March of 2022, after a period of organic growth and development, we initiated a collaborative process improvement project with IR aimed at reducing the number of direct-to-IR referrals for CVL, LP, paracentesis, and thoracentesis. Our initial intervention in March of 2022 was to establish an internal pathway for IR staff to encourage referring teams to refer procedures to the MPS on resource-constrained days. In June of 2022, our second intervention was to edit the IR consult wizard to directly involve the MPS for the target procedures.From January 2021 through October 2024, 1,742 procedures were referred directly to IR without MPS involvement. The number of procedures referred directly to IR without MPS involvement shows a marked decrease over time (Figure 1). Pre-implementation from January 2021 through March 2022, the average number of direct-to-IR procedures per month was 58 (range 38-70). Post-implementation, the average number of direct-to-IR procedures was 37.5 per month in the first 12 months (April 2022 through March 2023), 23 per month in the next 12 months (April 2023 through March 2024), and 20.4 per month from April 2024 through October 2024.
Conclusions: Hospital-wide implementation of an MPS combined with collaborative, multidisciplinary process improvement was associated with a progressive and sustained reduction in direct-to-IR referral rates for common bedside procedures. These findings highlight the potential of an MPS to optimize procedural resource management, providing a framework for IM and IR proceduralists, practice leaders, and hospital administrators considering MPS implementation.