Background: The delay or failure to follow-up test results pending at discharge (TRPAD) is a well-documented safety concern occurring in 20-61% of inpatients. Driving factors include ambiguity in the physician responsible and variable handoff practices between the inpatient and outpatient provider. Test result management encompasses many contextual factors such as clinical workflow, user behaviors, and organizational policies and procedures. Prior to this project, our institution did not have a standard process for management of TRPAD.
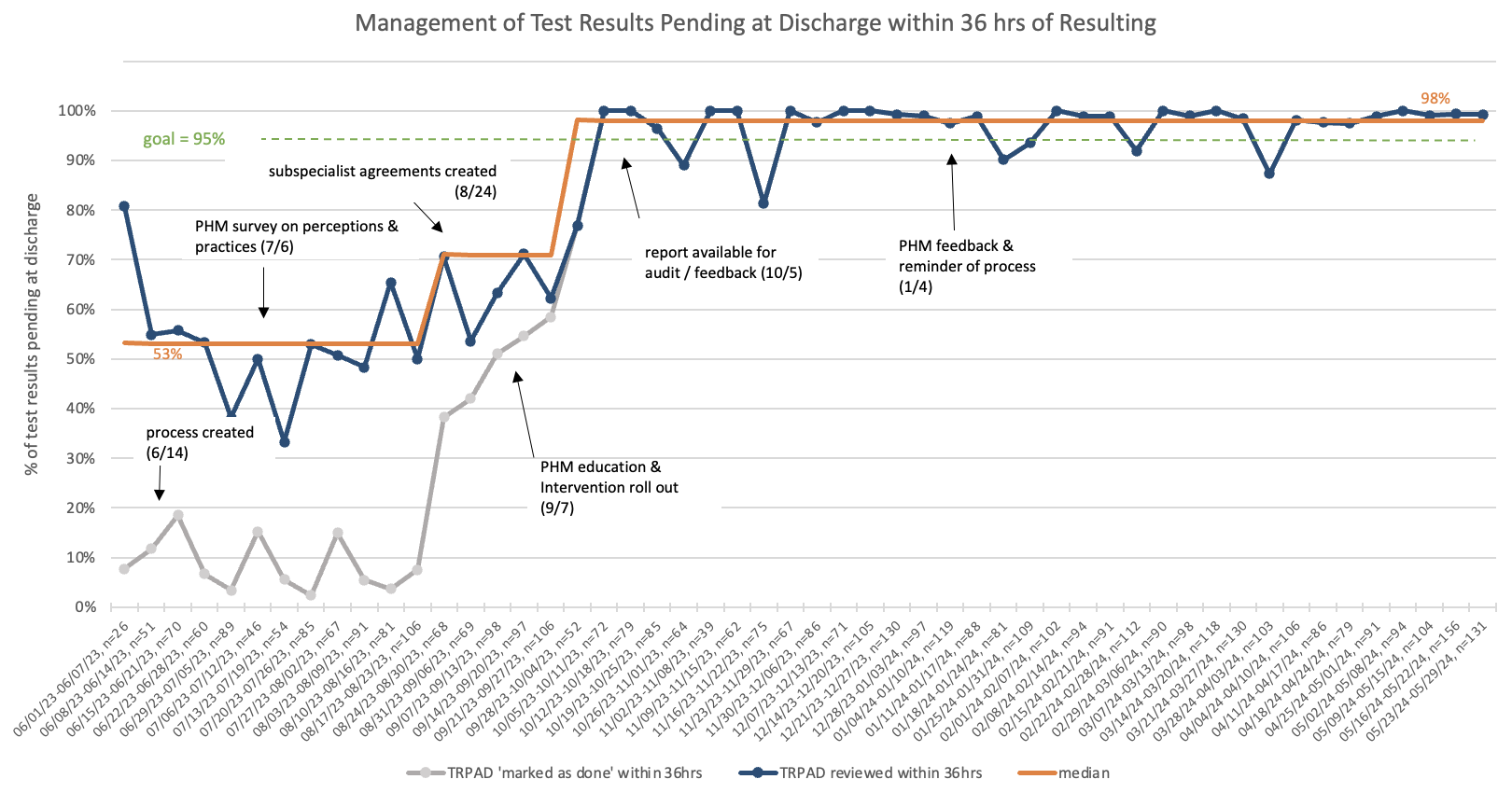
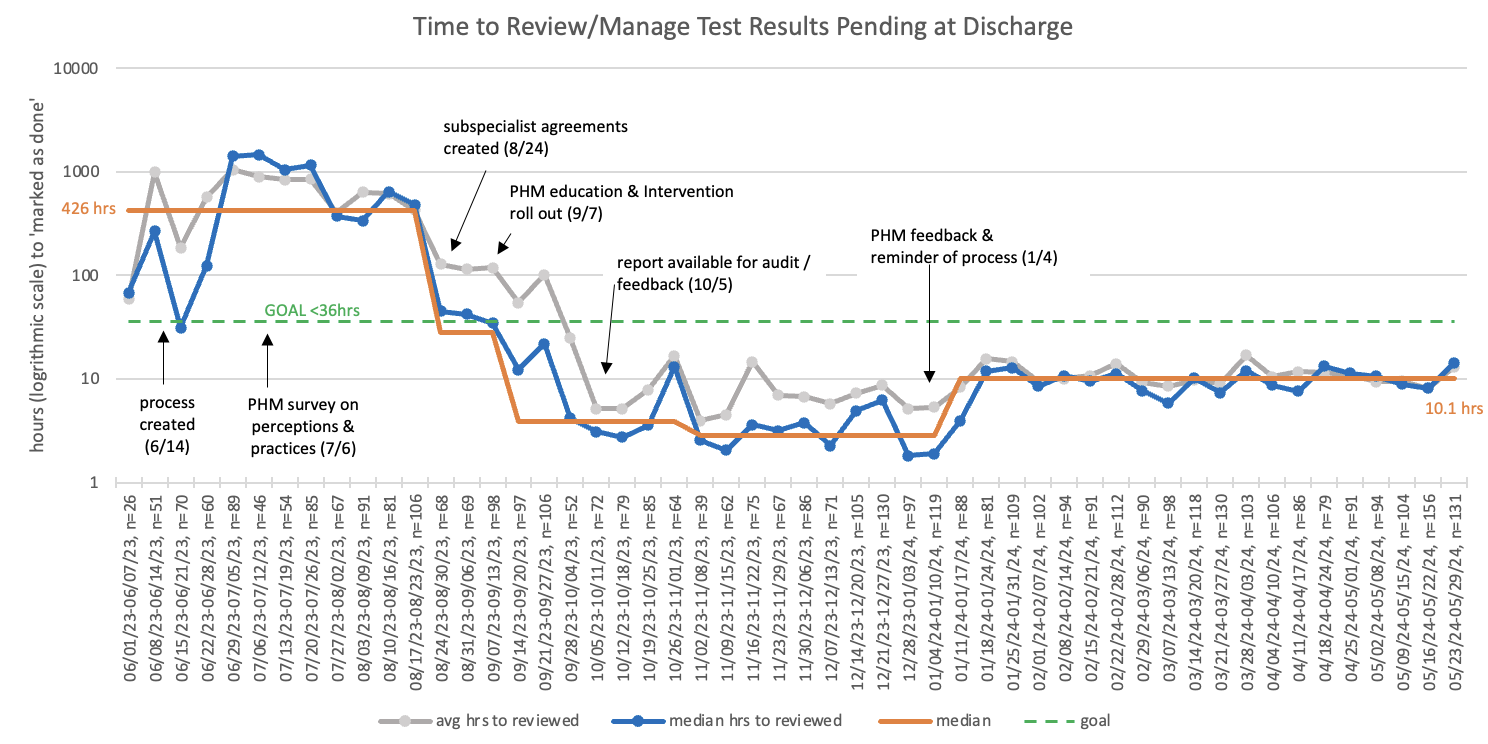
Purpose: We aim to increase the percentage of TRPAD for patients discharged by the pediatric hospital medicine (PHM) service that are managed within 36 hours of resulting from 53% to 95% in 3 months, and sustain improvement for an additional 9 months.
Description: The Model for Improvement was utilized. Measures included proportion of TRPAD managed within 36 hours (process), percentage with abnormal results (outcome), and time spent managing results (balancing). We created an in-basket shared pool within our EMR to which all TRPAD for patients discharged by the PHM service were routed. We then created a standard process that delegated the responsibility to manage results to the admitting physician. We set expectations for timing and a back-up plan for when the designated provider is unavailable. To standardize the process, we categorized TRPAD into four groups based on result type, effect on care plan, and urgency. A standardized workflow was developed for each category and supported by documentation templates and an instructional guide. Written agreements were also made with subspecialists on co-managing patient results.4530 TRPAD were reviewed, 1307 baseline and 3223 post-intervention results. TRPAD managed within 36 hours of resulting increased from a median of 53% to 98%. Median time to “mark result as done” decreased from 426 to 10.1 hours. 11% (n=369) of all TRPAD have been abnormal, with 4% of these (n=15) requiring an immediate change in management. Hospitalists spent an average of 10 minutes per day managing results within the shared pool. The designated hospitalist was unable to complete result management due to clinical responsibilities 16% (n=10 days) of the time.
Conclusions: Using Quality Improvement methodology, we achieved success in reducing the time to manage TRPAD and thus mitigating potential adverse patient outcomes. Post-intervention survey of the hospitalist group showed overall satisfaction with the new process. Next steps include improving patient portal communication and involving resident trainees in the process.